MCQ Type Questions for Midwives:
Question 1:
What is the main purpose of performing an episiotomy during childbirth?
A) To reduce maternal distress
B) To prevent cerebral damage in premature babies
C) To quicken delivery in certain cases
D) To prevent excessive bleeding
Answer: C) To quicken delivery in certain cases
Explanation: Episiotomy is a surgical incision made on the perineum to enlarge the vaginal orifice prior to delivery of the baby. It is performed to expedite the delivery process in specific situations, such as maternal distress, fetal distress, cord prolapse, rigid perineum, forceps delivery, face-to-pubis delivery, and certain other conditions.
Question 2:
Which type of episiotomy incision is discouraged due to the risk of damage to the Bartholin’s glands?
A) Medial lateral
B) J-shaped
C) Lateral incision
D) Bilateral
Answer: D) Bilateral
Explanation: The “bilateral” episiotomy incision is done on either side and is similar to the lateral incision. However, it is discouraged because it can cause injury to the Bartholin’s glands, which are located on either side of the vaginal opening.
Question 3:
What is the primary purpose of controlled cord traction during the third stage of labor?
A) To expedite placental delivery
B) To prevent perineal tears
C) To encourage maternal pushing
D) To reduce postpartum hemorrhage
Answer: A) To expedite placental delivery
Explanation: Controlled cord traction is a method used during the third stage of labor to help deliver the placenta more efficiently by applying controlled downward traction on the umbilical cord. It aims to shorten the duration of the third stage and reduce the risk of postpartum hemorrhage.
Question 4:
What is the average volume of blood flow through the placental site before the baby is born?
A) 100-200ml/min
B) 300-500ml/min
C) 500-800ml/min
D) 1000-1200ml/min
Answer: C) 500-800ml/min
Explanation: The normal volume of blood flow through the placental site before the baby is born is approximately 500-800ml/min. This blood flow decreases significantly once the baby is delivered and the placental separation begins.
Question 5:
Which stage of labor involves the separation, descent, and expulsion of the placenta and membranes?
A) First stage
B) Second stage
C) Third stage
D) Fourth stage
Answer: C) Third stage
Explanation: The third stage of labor involves the separation, descent, and expulsion of the placenta and membranes after the delivery of the baby.
Question 6:
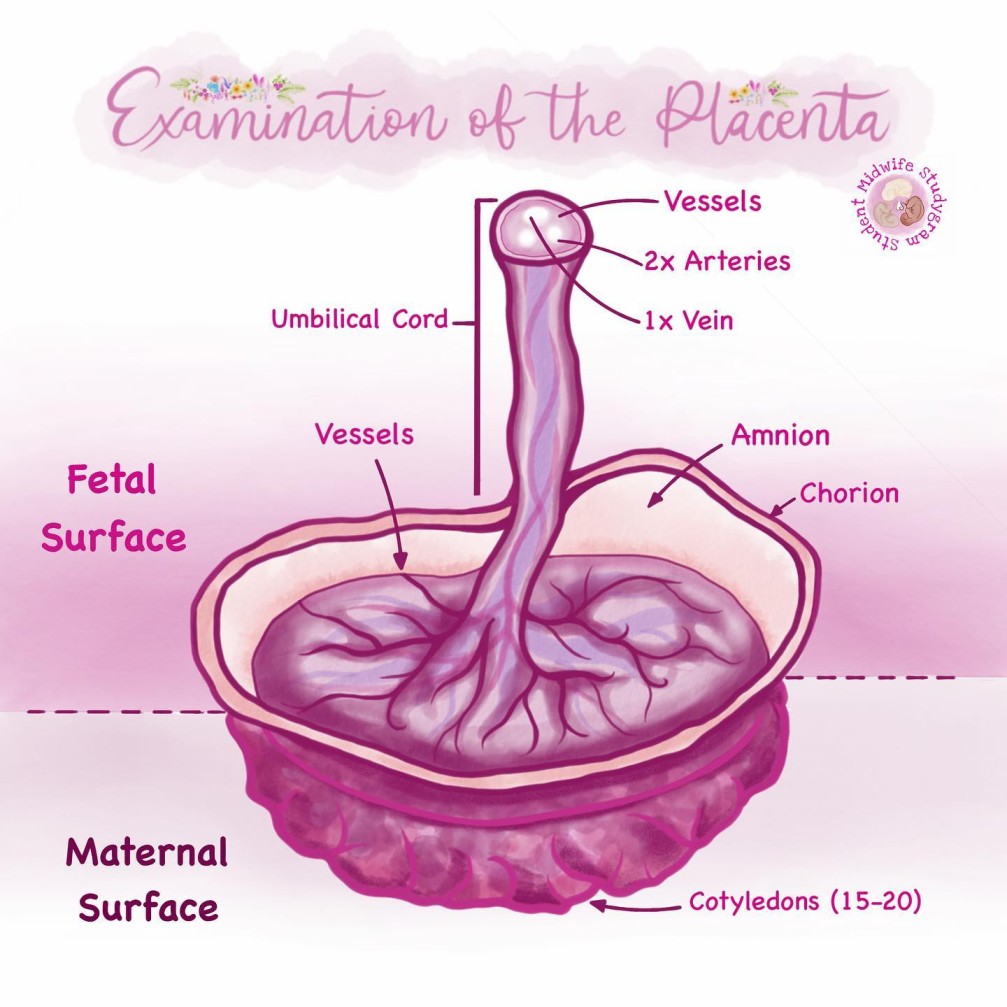
What is the main purpose of the placental examination after delivery?
A) To check the baby’s health status
B) To detect any abnormalities in the placenta
C) To ensure proper positioning of the baby
D) To assess maternal blood loss
Answer: B) To detect any abnormalities in the placenta
Explanation: The placental examination after delivery aims to assess the completeness of the placenta and membranes and to detect any abnormalities that may have occurred during pregnancy or delivery.
Question 7:
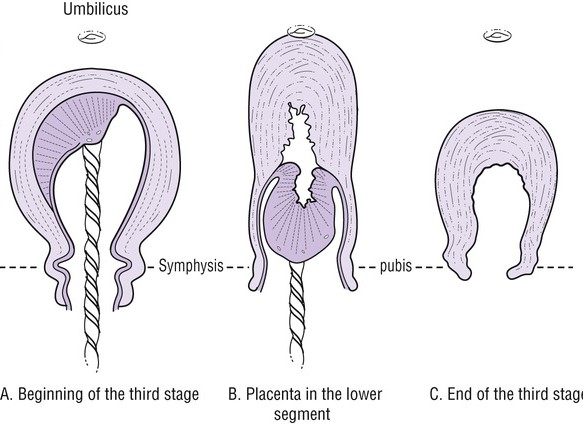
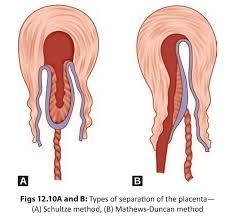
What is the recommended method of placental separation during the third stage of labor?
A) Mathew Dankan method
B) Active management with controlled cord traction
C) Passive management with maternal efforts
D) Schultze method
Answer: D) Schultze method
Explanation: The Schultze method is the recommended method of placental separation during the third stage of labor. It involves separation starting centrally, resulting in the formation of a retroplacental clot that aids in the separation process.
Question 8:
Which type of episiotomy incision is done by doctors and involves curving away from the anal sphincter?
A) J-shaped
B) Medial lateral
C) Bilateral
D) Lateral incision
Answer: A) J-shaped
Explanation: The J-shaped episiotomy incision is done by doctors and starts from the center of the fourchette, curving away from the anal sphincter.
Question 9:
What is the primary aim of uterine contractions during the third stage of labor?
A) To facilitate placental separation
B) To promote fetal descent
C) To prevent maternal discomfort
D) To dilate the cervix
Answer: A) To facilitate placental separation
Explanation: Uterine contractions during the third stage of labor help to facilitate placental separation and expulsion by reducing the area of the placental site and exerting pressure on the torn blood vessels.
Question 10:
Which stage of labor involves the arrest of hemorrhage?
A) First stage
B) Second stage
C) Third stage
D) Fourth stage
Answer: C) Third stage
Explanation: The third stage of labor involves the arrest of hemorrhage as the uterus contracts and closes the spiral arterioles after placental expulsion, reducing bleeding.
Question 11:
What is the main indication for performing an episiotomy in a forceps delivery?
A) To reduce fetal distress
B) To prevent cerebral damage in premature babies
C) To quicken delivery
D) To prevent excessive bleeding
Answer: C) To quicken delivery
Explanation: In a forceps delivery, an episiotomy may be performed to quicken delivery, allowing for easier extraction of the baby using forceps and reducing the risk of prolonged labor.
Question 12:
Which type of episiotomy incision is the commonest, safest, and recommended for use by midwives?
A) J-shaped
B) Medial lateral
C) Bilateral
D) Lateral incision
Answer: B) Medial lateral
Explanation: The medial lateral episiotomy is the commonest, safest, and recommended incision for use by midwives. It starts from the fourchette to the medial lateral direction of the perineum.
Question 13:
What is the typical healing time for an episiotomy?
A) 1-2 weeks
B) 2-4 weeks
C) 4-6 weeks
D) 6-8 weeks
Answer: C) 4-6 weeks
Explanation: The typical healing time for an episiotomy is around 4-6 weeks, depending on the size of the incision and the type of suture material used.
Question 14:
What is the average volume of blood flow through the placental site after the baby is born?
A) 100-200ml/min
B) 300-500ml/min
C) 500-800ml/min
D) 1000-1200ml/min
Answer: A) 100-200ml/min
Explanation: After the baby is born, the average volume of blood flow through the placental site reduces to approximately 100-200ml/min.
Question 15:
What is the primary aim of rubbing the fundus during the third stage of labor?
A) To assess the size of the uterus
B) To promote uterine contractions
C) To monitor the baby’s heart rate
D) To assess cervical dilation
Answer: B) To promote uterine contractions
Explanation: Rubbing the fundus during the third stage of labor helps to promote uterine contractions and assist in the expulsion of the placenta and membranes. It aids in preventing postpartum hemorrhage and achieving hemostasis.