
Normal Second Stage of Labour
1. Signs of the Second Stage
A midwife must closely observe the mother to know exactly when the second stage has started. The signs are divided into early warnings and one absolute confirmation.
Early Warning Signs (Premonitory Signs)
- Expulsive Uterine Contractions: The mother feels an uncontrollable urge to bear down and push. Note: This can sometimes happen before she is fully dilated, especially if the baby's head is facing her back (occipito-posterior) or if her rectum is full of stool.
- Rupture of Fore Waters: The bag of waters (amniotic sac) may break at this time, though it can happen earlier in labor.
- Dilatation and Gaping of the Anus: As the baby's head drops deep into the pelvis, it presses on the bowel, causing the anus to open wide (gape).
- Appearance of the Presenting Part: The baby's head becomes visible at the vaginal opening. Sometimes, heavy pressure causes a soft swelling on the baby's head (caput succedaneum) which can be seen even before the cervix is fully open. (In a breech birth, the buttocks might be seen when she is only 7-8cm dilated).
- Show: A sticky, blood-stained mucus plug comes out. The midwife must carefully check that this is a normal "show" and not dangerous bleeding from a tearing placenta.
- Congestion of the Vulva: The private parts become swollen, dark, and full of blood because of heavy pressure and early pushing.
- Bulging of the Perineum: The skin between the vagina and the anus stretches and bulges outward as the baby's head pushes against it.
Confirmatory Sign
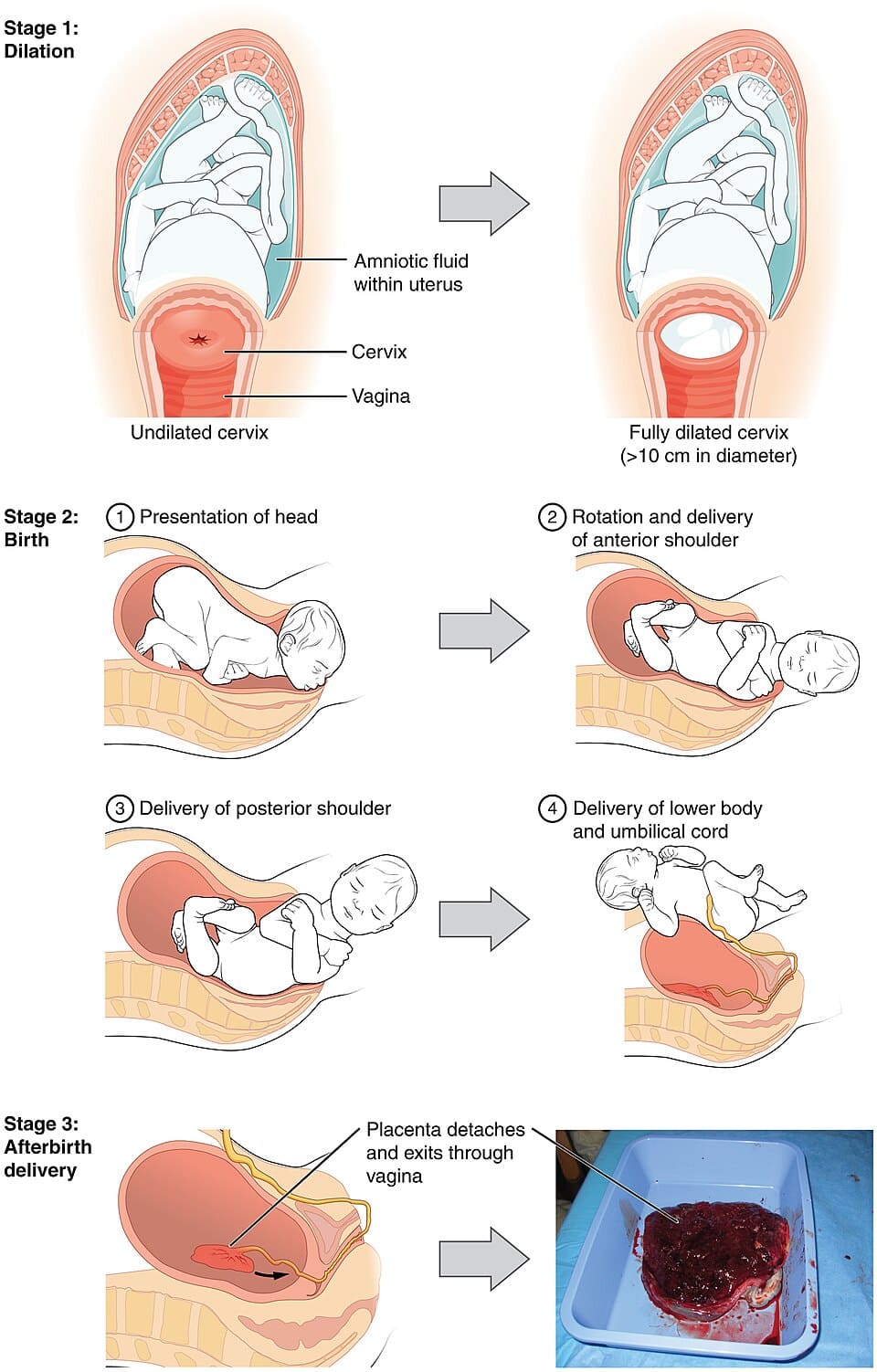
- No Cervix is Felt: When the midwife does a Vaginal Examination (VE), she can no longer feel the edges of the cervix. It is completely out of the way (full dilatation of 10cm). This is the only 100% sure sign.
Phases of the Second Stage
- Passive Phase: The cervix is fully open, but the mother's body is not yet forcing her to push (no involuntary expulsive contractions). In a healthy labor, this resting period can last up to one hour.
- Active Phase: The cervix is fully open, the body forces strong pushing contractions, and the baby is visible.
Time limits: You must inform a doctor if the baby is not born after 2 hours for a first-time mother (primigravida) or 1 hour for a mother who has delivered before (multigravida). - Propulsive Phase: The baby's head moves from the fully open cervix down to the bottom of the pelvis (pelvic floor).
- Expulsive Phase: The mother actively pushes with all her strength until the baby is completely delivered.
2. Physiology of the Second Stage
This explains exactly how the mother's body physically changes and reacts to push the baby out.
- Descent: The baby continues its rapid, downward journey through the pelvis until it hits the pelvic floor muscles.
- Uterine Action: Contractions become much stronger and longer. However, the breaks between them might get longer, giving the mother and baby time to recover (this rest can last up to an hour, especially for first-time mothers).
- When the water breaks, the hard round head of the baby presses directly on the vaginal tissue, which helps it stretch.
- The pressure of the baby's body pushing down bends the baby's neck (flexion), making the head smaller so it fits through the bones faster and safer.
- When the baby's head presses on the nerve receptors in the pelvic floor, it sends a powerful message to the mother's brain, causing an overwhelming urge to push. She responds by naturally tightening her stomach muscles and breathing muscle (diaphragm).
Soft Tissue Displacement (Moving Organs Out of the Way)
As the hard baby's head moves down, the soft organs inside the mother's pelvis are squeezed and pushed out of the way to prevent injury:
- Anteriorly (Front): The bladder is pushed high up into the abdomen to protect it from being crushed. This stretches the urine tube (urethra), making it very thin.
- Posteriorly (Back): The rectum (bottom bowel) is flattened flat against the backbone (sacrum). The heavy head pushes out any leftover stool (feces) as it passes.
- Pelvic Floor: The strong levator ani muscles stretch, thin out, and are pushed to the sides. The perineal body (skin between vagina and anus) stretches until it is paper-thin.
- Birth: The baby's head appears with each contraction and slips back slightly when the contraction stops, until it stays out (crowning). The head is born, followed by the shoulders and body, usually with a large splash of amniotic fluid and some blood.
3. Mechanism of Normal Labour
The mechanism of labour refers to the series of passive turns and movements the baby must make to successfully fit through the curves and tight spaces of the mother's pelvis.
🔑 Core Principles of the Mechanism
- Descent happens continuously throughout the whole process.
- Whichever part of the baby hits the pelvic floor muscles first will automatically rotate forward until it sits right under the pubic bone (symphysis pubis).
- The baby will pivot (swing) around the pubic bone to get out.
- The baby always turns its body to use the widest space available in the mother's bones.
Important Terms Used to Describe the Baby's Position
- Attitude: How the baby's head, arms, and legs are folded. The best attitude is "complete flexion" (chin tucked tightly to the chest), making the head as small as possible.
- Presentation: The part of the baby that is sitting lowest in the womb. The normal, safest presentation is "Vertex" (the top of the head).
- Lie: How the baby's spine lines up with the mother's spine. Normal labour requires a "Longitudinal" lie (spines are parallel), which happens 99.5% of the time.
- Presenting Part: The exact part of the baby sitting directly over the opening of the cervix.
- Denominator: The specific name of the bone used to describe the baby's position.
- Vertex presentation = Occiput (back of the head).
- Breech presentation = Sacrum (tailbone).
- Face presentation = Mentum (chin).
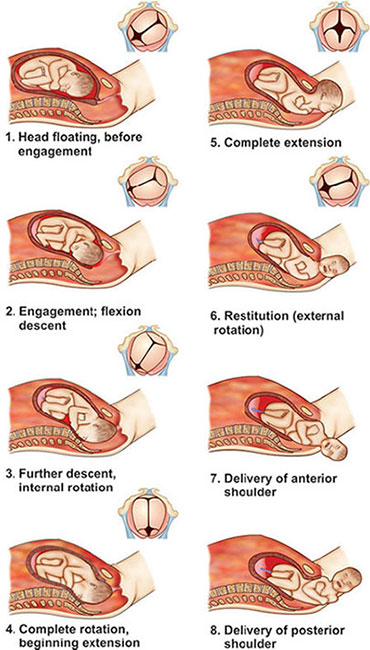
The 8 Main Movements of Labour
In a normal delivery (Cephalic presentation, Occiput denominator), the baby performs these steps in order:
- 1. Engagement: The widest part of the baby's head passes into the top of the pelvic brim. (Happens weeks before labour in first-timers, but late in labour for mothers who have delivered before).
- 2. Descent: The baby moves deeper down. This is pushed by strong uterine contractions, the mother bearing down, and the baby's body straightening out when the water breaks.
- 3. Flexion: The baby's head hits the walls of the pelvis, forcing the chin to tuck deeply into the chest. This reduces the presenting size from 10cm to a perfect 9.5cm.
- 4. Internal Rotation of the Head: The baby's head hits the pelvic floor muscles and turns slightly (1/8 of a circle) forward so the back of the head (occiput) sits under the mother's pubic bone.
- 5. Crowning: The widest part of the head pushes through the vaginal opening. It no longer slips back when the contraction stops. The head is about to be born.
- 6. Extension of the Head: The back of the baby's head pivots under the pubic bone. The baby lifts its chin, and the face, nose, and chin sweep over the perineum and are born.
- 7. Restitution: As soon as the head is completely out, it naturally untwists itself to realign with the shoulders still inside. The head turns exactly 1/8 of a circle back to where it started.
- 8. Internal Rotation of Shoulders & External Rotation of Head: The shoulders inside rotate to fit the widest part of the exit. As the shoulders turn inside, the baby's head (which is already outside) visibly turns to the side (External Rotation).
- 9. Lateral Flexion: The top shoulder slips under the pubic bone, the bottom shoulder sweeps out over the perineum, and the rest of the baby's body easily bends to the side (lateral flexion) and slides out.
4. Factors Influencing the Length of the 2nd Stage
Not every mother will push for the same amount of time. The speed depends on:
- Maternal Parity: Mothers who have given birth before usually have stretched tissues, so the baby comes out much faster than a first-time mother.
- Fetal Size: A very large baby takes much longer to squeeze through the pelvic bones.
- Force of Uterine Contractions: Weak contractions (uterine inertia) make the stage very long.
- Presentation & Position: If the baby is facing the mother's stomach instead of her back, it takes longer for the head to rotate.
- Pelvic Size: A narrow or deformed pelvis creates heavy resistance.
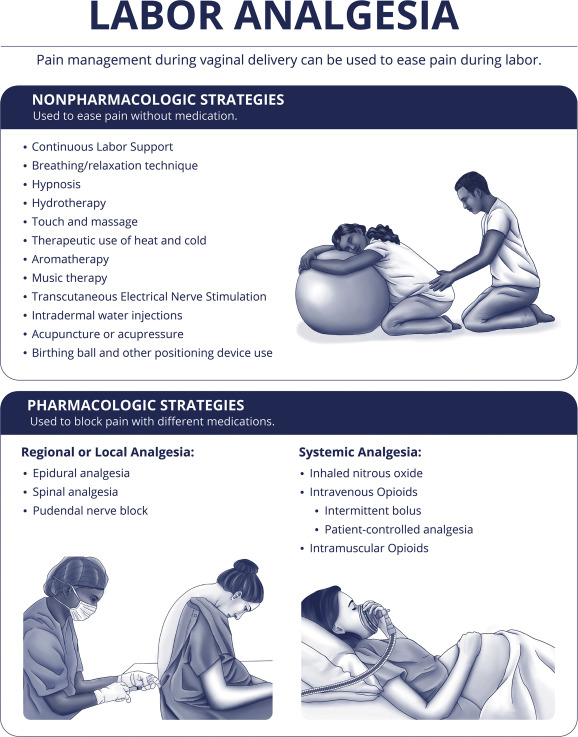
- Method of Anesthesia: Epidurals or heavy painkillers can numb the pelvic nerves, stopping the mother from feeling the urge to push strongly.
- Maternal Effort: How hard the mother is physically able to push, push correctly, and her emotional stamina.
5. Management & Nursing Care of the Second Stage
Basic Midwifery Care
- Bladder Care: Always encourage the mother to empty her bladder at the start of the second stage. A full bladder blocks the baby from dropping down and can be easily torn or crushed during birth.
- Hygiene and Comfort: Wipe away any stool or blood gently. Place a sterile pad over the vulva between contractions. If she gets leg cramps from pushing, massage the leg and gently bend it to relieve the pain.
- Emotional Support: Do not leave the woman alone. Praise her constantly, tell her she is doing a good job, and keep her updated ("I can see the baby's hair!"). Keep the room quiet, private, and calm to reduce her fear.
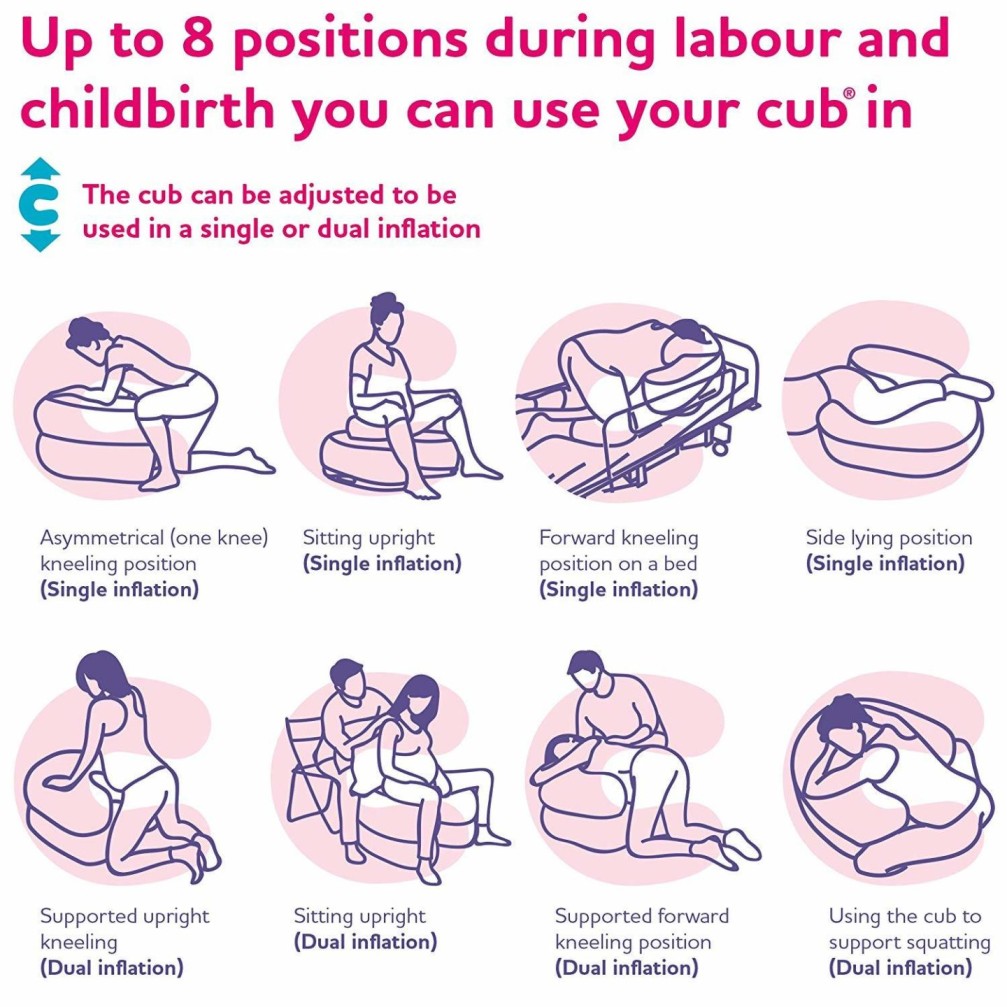
- Positioning: Let her choose the most comfortable position. This can be lying on her back (dorsal), squatting, kneeling, all fours, standing, or lying on her left side. Upright positions use gravity to help the baby come down faster.
- Observations: Constantly check her blood pressure (hourly) and pulse (every 30 mins). Watch the baby's heart rate, the color of the amniotic fluid (green means danger), and how well the mother is coping emotionally.
Requirements: Preparing the Delivery Trolley
The midwife must set up the delivery room long before the baby arrives. A sterile trolley is arranged in three areas:
| Top Shelf (Sterile Pack) | Bottom Shelf (Medicines & Supplies) | Beside the Bed / Room Setup |
|---|---|---|
|
|
|
6. Conducting the Delivery (Active Management)
Responsibilities of the Assistant Midwife
While the primary midwife delivers the baby, the assistant plays a massive role:
- Reassure and comfort the mother constantly.
- Help hold the mother in the correct pushing position.
- Instruct the mother *exactly* when to push (during the contraction) and when to pant/rest.
- Listen to the fetal heart rate immediately after every single contraction to ensure the baby is surviving the pressure.
- Give an injection of Oxytocin in the mother's thigh within 1 minute of the baby being born to stop heavy bleeding (Active Management of Third Stage).
- Show the sex of the baby to the parents.
- Score the baby's health (APGAR score) at 1 minute and 5 minutes.
- Dry the baby, keep it warm, and put it on the mother's chest for skin-to-skin contact and early breastfeeding.
Step-by-Step Delivery Procedure
- Preparation: Explain everything to the mother. Put on your protective gear (gum boots, plastic apron, and face mask). Position the mother properly.
- Scrubbing: Wash your hands thoroughly with soap and clean water to remove all bacteria. Put on two pairs of sterile gloves.
- Draping: Clean the mother's vulva with an antiseptic swab. Cover her legs and abdomen with sterile towels. Place a sterile pad tightly over her anus to prevent stool from dirtying the delivery area.
- Delivery of the Head:
- As the head pushes out, press two fingers gently on the top of the baby's head to keep the chin tucked to the chest (maintain flexion). This stops the head from bursting out too fast and tearing the mother.
- When the head stays out between contractions (Crowning), shout to the mother to STOP pushing and start panting like a dog. This allows the head to slide out smoothly and slowly.
- Gently guide the head upward toward the pubic bone to deliver the face and chin.
- Immediately wipe the baby's face, clean the eyes from the inside to the outside, and use a bulb syringe to suck mucus out of the nose and mouth.
- Quickly check if the umbilical cord is wrapped around the baby's neck. If it is loose, slip it over the head. If it is very tight, clamp it in two places and cut it immediately.
- Delivery of the Shoulders:
- Wait for the baby's head to naturally turn to the side (restitution/external rotation). This means the shoulders have turned into the correct position inside.
- Place your hands flat on the sides of the baby's head (over the ears).
- Pull gently downward to deliver the top (anterior) shoulder under the pubic bone.
- Then lift gently upward to deliver the bottom (posterior) shoulder over the perineum.
- The rest of the wet, slippery body will slide out easily. Place the baby directly onto the mother's belly or chest.
Immediate Care of the Newborn (The First Hour)
- Note the exact time of delivery.
- Clamp and cut the cord (if not already done). Tie it tightly with a clean ligature.
- Ensure the airway is totally clear. A strong, lusty cry is excellent as it forces the baby's lungs to pop open and expand.
- Dry the baby instantly to prevent heat loss. Wrap the baby in a sterile, warm towel.
- Place the baby on the mother’s bare breast (skin-to-skin) to bond and start breastfeeding.
- Calculate the APGAR score at 1 minute and again at 5 minutes.
- Show the mother the baby’s face and sex.
- Put a name tag on the baby's arm or leg showing the mother's name, sex, time, date, and weight.
- Cover the mother with a blanket to keep her warm.
7. Possible Complications of the Second Stage
The second stage is high-pressure. If it takes too long or if the baby gets stuck, severe emergencies can occur. The midwife must be ready to identify and manage:
⚠️ Danger Signs & Complications
- Deep Transverse Arrest: The baby's head gets completely stuck halfway turning inside the pelvis and refuses to rotate further.
- Obstetrical Shock: The mother collapses due to overwhelming pain, severe bleeding, or extreme exhaustion.
- Uterine Inertia: The uterus becomes entirely exhausted and the contractions become weak or stop completely.
- Maternal Distress: The mother becomes dehydrated, feverish, panicked, and physically unable to continue.
- Shoulder Dystocia: A terrifying emergency where the baby's head is born, but the shoulders get stuck behind the mother's pubic bone.
- 3rd-Degree Perineal Tear: The baby bursts out so fast or is so large that it tears the mother's vagina all the way down through the anal sphincter muscle (where stool comes out).
- Amniotic Fluid Embolism: A rare but deadly event where the baby's water (amniotic fluid) is pushed backward into the mother's bloodstream, causing her heart and lungs to collapse.
- Ruptured Uterus: The contractions are so violent, or the baby is so blocked, that the muscular wall of the uterus actually tears open.
- Fetal Distress: The baby runs out of oxygen. The fetal heart rate drops dangerously low or the baby passes green stool (meconium) into the water.

Interesting
work well done