
The Partograph & Management of 1st Stage of Labour
1. Introduction to the Partograph
A partograph is a graphical tool used strictly during the active first stage of labor. It is used to record important (salient) conditions of both the mother and the fetus to quickly detect any abnormalities so that immediate action can be taken.
Uses of a Partograph
- Detect Abnormal Progress: It helps the midwife quickly see if labor is not progressing or moving forward normally.
- Indicate Need for Augmentation: It shows exactly when it is appropriate to speed up (augment) labor using drugs like Oxytocin.
- Recognize CPD: It helps recognize Cephalopelvic Disproportion (CPD) when an obstruction occurs (meaning the baby's head is too big for the mother's pelvis).
- Improve Observation Quality: It increases the quality and accuracy of all observations made on the mother and fetus.
- Early Warning System: It serves as a strict visual alarm system for complications.
- Decision Making: It assists midwives in making early decisions to transfer the mother to a higher-level hospital or to assist the labor.
Who Should NOT Use a Partograph?
The partograph is for normal, active vaginal labor. It should not be used for:
- Women with major problems identified before or during labor who need special, constant doctor attention (e.g., severe bleeding, severe pre-eclampsia).
- Women who are not planning to have a vaginal delivery (e.g., those scheduled for an elective Caesarean Section).
2. Starting the Partograph
The partograph must only be started when the woman enters the Active Phase of Labour. You know she is in the active phase when:
- Her cervical dilatation is 4cm or more.
- She is having 1 or more true contractions in 10 minutes.
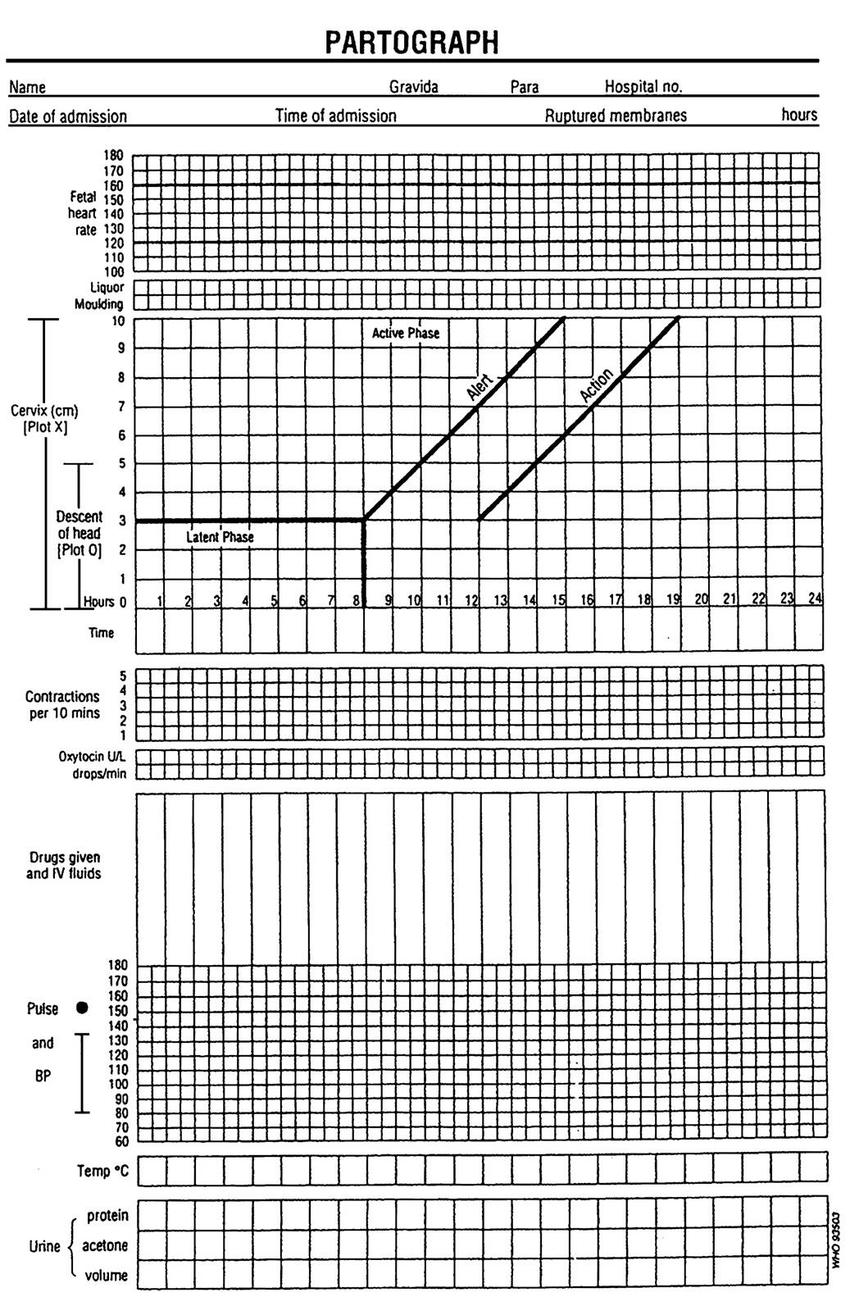
The 3 Main Parts of a Partograph
Every standard partograph is divided into three distinct sections that must be closely monitored:
- 1. Fetal Condition Part: Monitors the baby's wellbeing.
- 2. Labour Progress Part: Monitors how fast the cervix is opening and the baby is dropping.
- 3. Maternal Condition Part: Monitors the mother's vital signs and strength.
3. Monitoring the Fetal Condition
This section is purely to ensure the baby is surviving the stress of labor contractions safely.
- Fetal Heart Rate (FHR): Taken every ½ hour (30 minutes). The normal FHR is 120-160 beats per minute. If it is below 120 or above 160, it indicates fetal distress. If it is abnormal, you must check it more frequently (every 15 minutes). If it remains abnormal over 3 observations, you must take immediate action.
Moulding of the Fetal Skull (Checked 4-hourly)
Moulding is the normal overlapping of the baby's skull bones to allow the head to fit through the narrow birth canal. It is felt during a Vaginal Examination (VE) and plotted using specific grades:
| State of Moulding | Record Symbol | Midwife Interpretation |
|---|---|---|
| Absence of moulding | (-) | Normal. The head fits easily. |
| Bones separate, sutures felt | (0) | Normal. Bones are not touching yet. |
| Bones just touching | (+) | Normal moulding has started. |
| Bones overlapping but separable | (++) | Moderate. The bones can still be pushed apart with a finger. |
| Bones overlapping, inseparable | (+++) | Danger (Severe Moulding). Indicates the baby's head is completely stuck (CPD). |
State of Liquor Amnii & Membranes (Checked 4-hourly)
When the bag of waters (membranes) breaks either naturally (spontaneously) or by the midwife (artificially), the water (liquor) is observed.
| State of Liquor (Water) | Record Symbol | State of Membranes | Record Symbol |
|---|---|---|---|
| Clear (Normal) | (C) | Membranes Intact | (I) |
| Light green (Meconium stained) | (m+) | Membranes Ruptured | (R) |
| Moderate green, more slippery | (m++) | ||
| Thick green, heavily stained | (m+++) | ||
| Blood stained | (B) |
*Note: Meconium is the baby's first stool. If the baby passes it inside the womb (green liquor), it is a major sign that the baby is struggling to breathe or is in distress.
4. Monitoring Labour Progress
This section tracks the physical work of labor: the cervix opening, the baby dropping, and the uterus squeezing.
- Cervical Dilatation (Checked 4-hourly): Measured in centimeters. It is plotted with an "X" on the graph. A vaginal examination is done on admission and once every 4 hours. Recording starts exactly at 4cm.
⚠️ The Alert and Action Lines
- Alert Line: Starts at 4cm and goes diagonally upward at a rate of 1cm per hour. If the plotted "X" crosses to the right of this line, it is an alert that labor is slowing down.
- Action Line: Drawn parallel to the Alert line, exactly 4 hours to the right of it. If the plot reaches this line, medical action (like a C-Section or giving Oxytocin) MUST be taken immediately.
- Descent of Presenting Part (Checked 2-hourly): Checked by feeling the mother's abdomen (abdominal palpation). It is measured in "fifths" above the pelvic brim using the width of the midwife's five fingers. It is plotted with an "O" on the graph.
- If the head is loose (ballotable) above the brim, it accommodates all 5 fingers (5/5).
- As the head drops down (descends), fewer fingers can feel it above the pelvic bone.
- The head is considered fully engaged when only 2 or fewer fingers can feel it above the brim (2/5 or less).
- Uterine Contractions (Checked every 30 mins): The midwife must feel the mother's belly for exactly 10 minutes to count how many contractions happen, how long they last (duration), and how strong they are.
- Mild: Lasts for less than 20 seconds. (Plotted using Dots).
- Moderate: Lasts for 20-40 seconds. (Plotted using Diagonal lines).
- Strong: Lasts for 40 seconds or more. (Plotted using full Dark Shading).
5. Monitoring the Maternal Condition
The mother works extremely hard during labor. Her physical signs must be tracked to ensure she does not collapse from exhaustion or infection.
- Pulse (Every 30 mins): Normal is 70-90 beats/min. A raised pulse may indicate maternal distress, bleeding, or infection (especially if her waters broke 8-12 hours ago). A very low pulse can mean the mother is collapsing.
- Blood Pressure (Every 2 hours): Normal is between 90/60 and 140/90 mmHg. If the top number (systolic) rises by 30 or the bottom (diastolic) rises by 20 above her normal, or stays high for 3 readings, test her urine for albumen to check for dangerous Pre-Eclampsia.
- Temperature (Every 4 hours): Normal is 37.2°C to 37.5°C. A high fever means infection, dehydration, or maternal distress, especially common if the membranes ruptured very early.
- Urine (Every 2 hours): The mother should pass urine at least every 2 hours. Test the urine on admission for Volume, Acetone (shows starvation/dehydration), Proteins (shows Pre-Eclampsia), and Sugars (shows Diabetes).
- Fluids and Drugs: Record any IV fluids given (2-hourly), the Oxytocin regimen (if used to speed up labor), and any pain drugs given. The mother should be encouraged to drink 250-300 mls of sweetened fluid every 30 minutes to keep her energy up (no alcohol).
6. Further Management in the Normal 1st Stage of Labour
Proper nursing care is critical during the active first stage to keep the mother comfortable, safe, and progressing normally.
Comprehensive Nursing Care
- 1. Emotional Support & Pain Relief: The midwife should rub the mother's lower back to relieve contraction pain. Keep the mother reassured and constantly informed about her progress to reduce fear and anxiety. Allow her to move around, talk to her relatives or husband, or do light activities like reading or knitting.
- 2. Nutrition: Labor burns massive amounts of energy. Encourage the mother to take light, easily digested foods like bread, soup, and warm sweet tea. This prevents dehydration and gives the uterine muscles the energy they need to contract strongly. Heavy foods should be avoided as the stomach empties very slowly during labor.
- 3. Elimination (Bladder and Bowel Care): A full bladder blocks the baby's head from dropping down. Encourage the mother to urinate every 2 hours. Every single urine sample is measured and tested for acetone, albumen, and sugars, and the results are recorded. If the mother absolutely cannot pass urine herself, the midwife must carefully pass a catheter to empty it.
- 4. Personal Hygiene: Allow the mother to take a warm bath in early labor to relax. Once her waters (membranes) rupture, give her a clean sanitary pad and ask her to change it frequently to stop bacteria from entering. Vaginal examinations (VE) must strictly be done using sterile, aseptic techniques.
- 5. Ambulation (Walking) and Position: In early labor, encourage the mother to walk around. Gravity helps the baby's head drop down (descent). During strong pains, ask her to lean forward on a chair or the bed to reduce back discomfort. She can choose any comfortable position except the flat supine (flat on her back) position, which drops her blood pressure. Once the membranes rapture deeply into advanced labor, she should stay in bed.
- 6. Prevention of Infections: Strict cleanliness (aseptic technique) must be maintained when checking the cervix or swabbing the vulva. If the waters break early, clean the vulva every 4 hours. The doctor may start antibiotics to stop bacteria from traveling up to the baby (ascending infection). Wash the mother with a sponge and change dirty bed sheets to keep her comfortable. The midwife must always wash her hands before and after touching the mother.
- 7. Sleep and Rest: Labor is exhausting. Strongly encourage the mother to rest, close her eyes, and breathe deeply in between the contractions to save her energy for the final pushing stage.
7. What to Report (Danger Signs)
The midwife must immediately report any of the following warning signs to the doctor in charge:
- Any abnormal substances found in the urine (high protein, high acetone).
- Total failure of the mother to pass urine.
- A sudden spike in the mother's temperature, pulse, or blood pressure.
- Hypertonic uterine contractions (contractions that are too strong, too long, and never give the uterus time to rest).
- Membranes rapturing with thick, meconium-stained liquor (Grade 2 and Grade 3).
- Failure of the baby's head to drop down (descend) even though the mother has strong, good contractions.
- Severe, constant tenderness over the abdomen (warning sign of a tearing uterus).
- Fresh bleeding from the vagina (Bleeding per vagina).
- A sudden, dangerous drop in blood pressure (Fall in BP).
- A highly raised or severely dropped fetal heart rate.
Complications of the 1st Stage of Labour
If the first stage is not managed well, the following severe complications can arise:
| Complication | Brief Explanation (Extra Midwifery Detail) |
|---|---|
| Infections | Bacteria entering the open cervix, especially if membranes ruptured hours ago. |
| Early Rupture of Membranes | The water breaking way before the cervix is fully open, risking infection. |
| Cord Prolapse | The umbilical cord slips out of the cervix before the baby, cutting off the baby's oxygen. |
| Supine Hypotensive Syndrome | Mother's blood pressure crashes because she is lying flat on her back. |
| Fetal Distress | The baby is running out of oxygen, shown by abnormal heart rate and green liquor. |
| Maternal Distress | The mother is totally exhausted, dehydrated, and has a high pulse/fever. |
| APH (Antepartum Haemorrhage) | Severe bleeding before the baby is born (e.g., placenta separating early). |
| PET and Eclampsia | Extremely high blood pressure leading to dangerous maternal seizures (fits). |
| Prolonged Labour | Labor taking much longer than normal, crossing the Partograph Alert Line. |
| Obstructed Labour | The baby physically cannot pass through the bones, crossing the Partograph Action Line. |

This was so helpful thank you very much for simplifying my revision
Can i have a question example about a pantograph and how the information can be plotted on the pantograph?
Thank you
Quite good
I have sincerely enjoyed this revision notes
so helpful..I love reading this simplified approach