
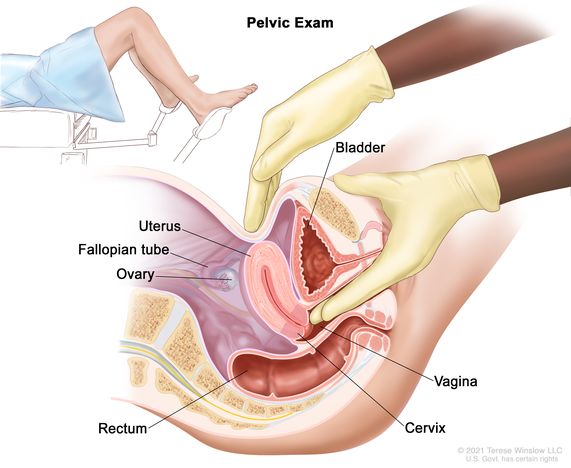
Internal Pelvic Assessment
Internal pelvic assessment is usually done around 36 weeks of pregnancy for first-time mothers (primigravida) or by a midwife during labor. This assessment helps determine if the pelvis can accommodate the baby during delivery.
Scenario
A mother who is pregnant for the third time (Gravida 3, Para 1) arrives with labor pains. Your task is to perform a pelvic assessment to evaluate pelvic capacity.
Objectives
- Prepare the necessary equipment for an internal pelvic assessment.
- Conduct the internal pelvic assessment for the mother in labor.
Requirements
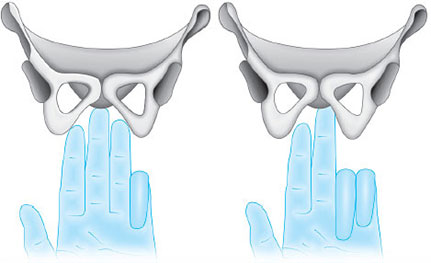
NOTE: Measure the length of your fingers from the curve of the thumb to the middle finger, to measure the diagonal conjugate.
Procedure



Note:
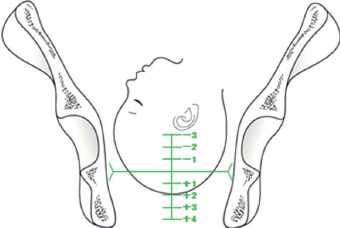
During labour, while performing pelvic assessment, also assess the station of the fetus. Stations indicate how far the fetus has descended into the pelvis and can be felt during a vaginal examination, especially at stations -3, -2, and -1.
Station Table:
The table represents fetal station measurements during labor, which describe the position of the fetus’s presenting part (usually the head) in relation to the maternal ischial spines.
The ischial spines are bony protrusions in the pelvis and serve as a key landmark in determining the station.

thanks for good work