
Fibroids (Fibromyomas)
Uterine Fibroids are benign (non-cancerous) tumors that originate from the smooth muscle layer (myometrium) of the uterus.
- Other Medical Names: Uterine leiomyoma, myoma, fibromyoma, and fibroleiomyoma.
- Demographics: They typically occur after the age of 30 years and are most commonly seen in nulliparous women (women who have never had children).
- Characteristics: They are composed of dense muscle and fibrous tissue. They can be single or multiple, and range in size from a tiny microscopic pinhead to an enormous mass that distorts the entire abdomen. They are far more likely to arise in the body of the uterus than in the cervix.
Risk Factors for Uterine Fibroids
While the exact primary cause is still being researched, several established clinical risk factors drastically increase a woman's likelihood of developing uterine fibroids:
- Age: Fibroids are most prevalent and aggressively grow in women between the ages of 30 to 40 years.
- Parity (Number of Pregnancies): Women who are nulliparous (have never given birth) or have very low parity are at a significantly higher risk. Pregnancy seems to have a protective effect.
- Race / Ethnicity: Uterine fibroids are disproportionately more prevalent, tend to appear at a younger age, and grow larger in individuals of African descent (Black women) compared to those of Caucasian (White) ethnicity.
- Family History: Genetics play a strong role. If a woman has close first-degree relatives (such as a mother or sister) with a history of fibroids, her personal risk is highly increased.
- Hyper-estrogenemia: Elevated levels of the female hormone estrogen directly promote the rapid growth of fibroids. Fibroids are highly estrogen-dependent.
- Obesity: Being overweight or obese is strongly associated with a higher risk. (Pathophysiology note: Adipose/fat tissue converts androgens into estrogen, leading to higher overall circulating estrogen levels).
- Early Onset of Menarche: Starting menstruation at a very young age (early exposure to cyclic hormones) is linked to an increased likelihood of fibroid development later in life.
- Low Level of Vitamin D: Recent clinical studies suggest that a deficiency or insufficient levels of Vitamin D might be associated with a higher risk of fibroid growth.
- Drugs (Estrogen Replacement Therapy): Long-term use of estrogen replacement therapy, particularly when used without progesterone to balance it, acts as a direct catalyst for fibroid growth.
Classes, Types, and Locations of Uterine Fibroids
Fibroids are classified based on their specific growth patterns and exactly where they are situated within or around the uterus.
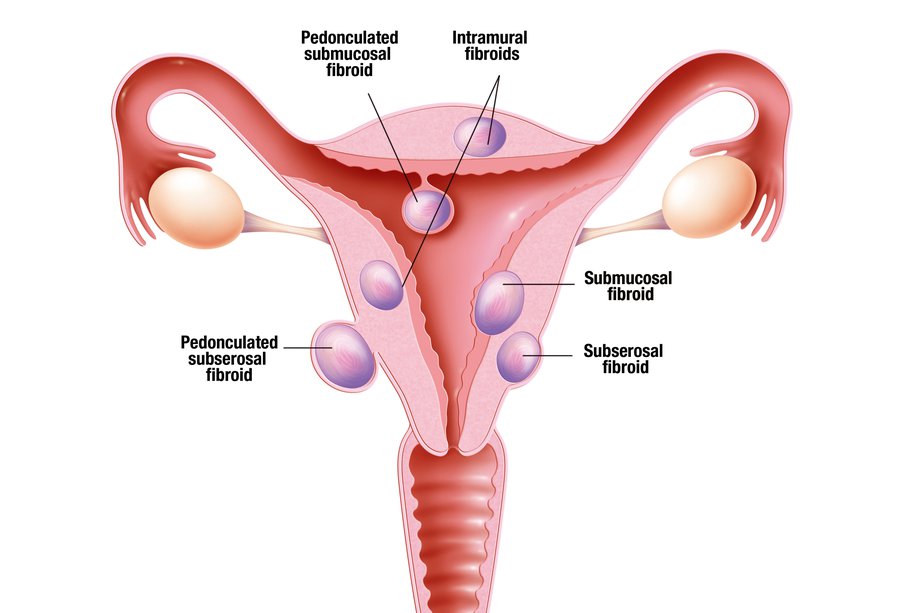
1. Types of Uterine Fibroids
The "type" refers to the specific category based on its growth characteristic relative to the uterine layers:
- Submucosal Fibroids: These grow directly into the uterine cavity, situated just beneath the inner lining (endometrium). Because they disrupt the cavity, they are the main culprits for heavy menstrual bleeding (menorrhagia) and infertility.
- Intramural (Interstitial) Fibroids: The most common type. They grow centrally within the thick muscular wall of the uterus (myometrium). As they expand, they distort the overall shape of the uterus, leading to severe pain and pressure.
- Subserosal Fibroids: These grow on the outside surface of the uterus, just under the serosa layer. They project outward into the pelvic cavity, often growing quite large and pressing on nearby organs like the bladder or rectum.
- Pedunculated Fibroids: These are attached to the uterus by a narrow stalk or pedicle that contains their blood supply. They can be either pedunculated subserosal (hanging outside) or pedunculated submucous (hanging inside the cavity).
- Cervical Fibroids: Located specifically on the cervix (the lower neck of the uterus). These are relatively rare but can cause severe pain, discomfort, and major complications (like obstructed labour) during childbirth.
- Fibroid of the Broad Ligament: Develops outward into the broad ligament (the supportive structure holding the uterus in place). They are uncommon and require very specific surgical management to avoid damaging the ureters.
Understanding the Difference: Types vs. Location
Many students confuse "Types" with "Location." Here is the clinical distinction:
| Concept | Definition | Examples |
|---|---|---|
| Types of Fibroids | Refers to the different categories or classifications based on their specific growth patterns and characteristics. | Submucous, Intramural, Subserosal, Pedunculated, Cervical. |
| Location of Fibroids | Refers to the specific physical site within or around the pelvic organs where the fibroid has situated itself. Location dictates which organs it will press against. | Subperitoneal (under peritoneal surface), Bulging into the endometrial cavity, Centrally within the myometrium, At the outer border, On the cervix. |
Statistical Frequencies and Specific Positions
- Intramural / Interstitial: Accounts for the vast majority at 75%. Initially intramural, they may later be pushed outward or inward, but about 70% persist in this central position.
- Subserous / Subperitoneal: Accounts for 15%. They are pushed outward towards the peritoneal cavity and are either partially or completely covered by the peritoneum.
- Submucous: Accounts for only 5%. Despite being the least common, it produces the maximum number of symptoms.
- Cervical Positions: Depending on exactly where they grow on the cervix, they are classified as: Anterior, Posterior, Lateral, or Central cervical fibroids.
Pathology and Microscopic Structure
Understanding the exact cellular structure of a fibroid helps explain its surgical and clinical behavior:
- Gross Pathology: Fibroids are firm, spherical, or irregularly lobulated. They possess a false capsule (pseudocapsule) made of areolar tissue and compressed normal myometrium. Because the capsule is false, the fibroid can be easily "enucleated" (shelled out) from the surrounding myometrium during surgery.
- Microscopic Structure: Consists of smooth muscle cells that are spindle-shaped and uniform. They are arranged in a distinct whorled pattern interlaced with varying amounts of fibrous connective tissue.
- Vascularity: Arteries inside the fibroid are less dense than the surrounding myometrium and lack a regular distribution pattern. Usually, only 1 to 2 major vessels are found at the base or pedicle supplying the entire mass.
Changes in Surrounding Pelvic Organs
- The Uterus: The shape becomes grossly distorted. Myohyperplasia (overgrowth of muscle cells) is a constant finding. There is massive dilatation and congestion of the myometrial and endometrial venous plexuses. The uterine cavity itself may become elongated and distorted.
- The Ovaries: Often become enlarged, highly congested, and studded with multiple cysts. Anovulation is commonly associated.
- The Ureters: Broad ligament fibroids cause severe displacement of normal ureter anatomy, increasing the risk of surgical injury.
- Associated Conditions: There is a highly increased clinical association with pelvic endometriosis, adenomyosis, and endometrial carcinoma.
Causes of Uterine Fibroids
The exact trigger that causes a single smooth muscle cell to mutate and multiply into a fibroid is not fully understood, but clinical research points to two major driving forces:
- Hormones (Estrogen and Progesterone): These two hormones, which naturally regulate the menstrual cycle and thicken the endometrium, directly stimulate the growth of fibroids. Fibroids possess more estrogen and progesterone receptors than normal uterine muscle cells. Consequently, fibroids grow rapidly during the reproductive years (especially during pregnancy when hormone levels are massive) and naturally shrink (atrophy) during menopause when hormone production ceases.
- Genetics: Genetic alterations are frequently found in fibroid cells. A strong familial link exists; women with a mother or sister who had fibroids are genetically predisposed to developing them.
- Other Contributing Factors: Diet (high in red meat, low in green vegetables), obesity, and race (African descent) act as strong secondary catalysts.
Degenerative Changes in Uterine Fibroids
Because fibroids grow so rapidly, they often outgrow their own blood supply. When this happens, the tissue undergoes "degenerative changes" (alterations in tissue structure):
- Hyaline Degeneration: The most common type. The firm muscle fibers are gradually replaced by a soft, homogenous, structureless hyaline material. The most common type, occurring in 65% of cases affecting all sizes (except tiny ones). The tumor loses its firm feel and becomes soft and elastic. Naked-eye examination of a cut surface shows irregular, glassy, homogenous areas with a complete loss of the normal "whorl-like" appearance.
- Cystic Change: This usually follows hyaline degeneration. The soft hyaline tissue liquefies, leaving fluid-filled cavities that make the fibroid look exactly like an ovarian cyst.
- Red (Carneous) Degeneration: Occurs mainly in the second half of pregnancy and puerperium. Microscopically: shows evidence of severe necrosis. Odor & Color: It emits a distinct "fishy" odor due to fatty acids, and the raw-beef color is due to the presence of haemolysed red blood cells and hemoglobin trapped in the cystic spaces.
- Fatty Change: The muscle fibers of the fibroid are slowly replaced by fat (adipose) tissue.
- Atrophy: Following menopause, due to the drastic drop in estrogen and progesterone, the fibroid simply wastes away and shrinks in size.
- Calcification: Calcium salts are heavily deposited into the fibroid tissue, causing it to harden.
- Eggshell Fibroid: Calcium deposits form a hard shell strictly on the outside, leaving the inside soft.
- Womb Stone: The entire fibroid is completely infiltrated with calcium salts, becoming solid and hard like an actual stone.
- Septic / Infective Degeneration: Infection gains access to the tumor through thinned, sloughed surface epithelium of a submucous fibroid. This usually happens immediately following delivery or an abortion.
- Sarcomatous (Malignant) Change: The rarest but deadliest change. The benign fibroid undergoes malignant transformation into a leiomyosarcoma. This must be heavily suspected if a fibroid suddenly grows rapidly, especially in post-menopausal women.
- Parasitic Fibroid: Occurs when a pedunculated fibroid twists on its pedicle (torsion), completely cutting off its original blood supply. To survive, it attaches itself to nearby organs (like the omentum or bowel) and establishes a brand new "parasitic" blood supply from them.
🧠 Memory Aid: Degenerative Changes of Fibroids
Remember the letters: H - C - C - R - F - S - S
H = Hyaline (Most common, 65%)
C = Cystic (Liquefaction)
C = Calcific (Womb stone in menopause)
R = Red / Carneous (During pregnancy)
F = Fatty (Post-menopause)
S = Septic / Infective (Post-delivery/abortion)
S = Sarcomatous (Malignant transformation)
⚠️ Attention: Red Degeneration (Obstetric Emergency)
Red Degeneration is an acute complication that almost exclusively occurs during pregnancy. The fibroid grows so fast that its blood supply fails, leading to massive tissue necrosis (cell death) and hemorrhage inside the fibroid. It becomes soft, reddish, and looks like "beefy" raw meat. It causes the pregnant mother sudden, severe, localized abdominal pain, localized tenderness, and low-grade fever.
Clinical Presentation (Signs and Symptoms)
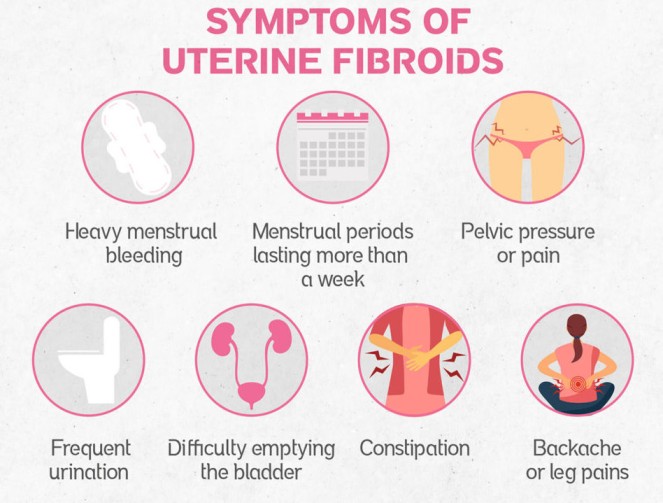
Many women with fibroids are asymptomatic. However, depending on the size, number, and location, they can present with severe symptoms:
- Menstrual Abnormalities:
- Painful & Prolonged Menstruation: Heavy menstrual bleeding (menorrhagia) and extremely painful periods (dysmenorrhea).
- Postmenopausal Bleeding: Vaginal bleeding occurring after menopause is highly abnormal and requires immediate investigation.
- Bulk and Pressure Symptoms:
- Urinary Issues: Anterior fibroids pressing against the bladder cause increased frequency of urination or difficulty emptying the bladder (retention).
- Constipation: Posterior fibroids pressing on the rectum block the passage of stool.
- Pelvic Pressure/Fullness: A constant feeling of heaviness or pressure in the lower abdomen.
- Abdominal Enlargement: Large or multiple fibroids can cause the abdomen to distend, mimicking the appearance of a pregnancy.
- Vascular Pressure: Extreme pelvic vein pressure can cause the development of severe hemorrhoids and varicose veins in the legs.
- Pain and Discomfort:
- Lower Back and Leg Pain: Caused by large fibroids pressing directly on pelvic nerves.
- Dyspareunia: Deep pain or discomfort during sexual intercourse.
- Acute Pain: Sudden, severe pain indicates a complication such as acute red degeneration or torsion (twisting) of a pedunculated fibroid.
- Reproductive Issues:
- Infertility: Submucosal fibroids distort the uterine cavity, physically blocking fallopian tubes or preventing the proper implantation of a fertilized egg.
Specific Symptom Triggers
- Dysmenorrhea Types: Can present as Congestive (due to massive associated pelvic venous congestion or endometriosis) or Spasmodic (associated with the violent uterine contractions attempting to expel a submucous polyp from the cavity).
- Extreme Urinary Retention: Rarely, a specific posterior fundal tumor can cause an extreme retroflexion of the entire uterus, violently distorting the bladder base and causing acute urinary retention.
- Bowel Obstruction: A parasitic fibroid that has detached and attached to the bowel can cause direct mechanical bowel obstruction.
- Cervical Symptoms: Tumors strictly on the cervix heavily provoke foul vaginal discharge, severe bleeding, and dyspareunia.
Diagnosis and Investigations
Diagnosing uterine fibroids involves a combination of thorough clinical examination and advanced imaging.
1. Clinical Examination
- History Taking: Comprehensive assessment of menstrual patterns, volume of blood loss, reproductive history, and pain levels.
- Physical Examination: Checking the patient's general health, specifically looking for signs of chronic anemia (extreme pallor of the conjunctiva and palms) resulting from prolonged menorrhagia.
- Abdominal Examination: Palpating the abdomen to detect large, firm, irregular pelvi-abdominal swellings rising out of the pelvis.
- Pelvic & Bimanual Examination: A two-handed examination to feel the size, shape, nodularity, and mobility of the uterus. A speculum examination may reveal fibroid polyps protruding directly through the cervical os.
2. Medical Investigations (Labs & Imaging)
- Pregnancy Test: A mandatory first step to rule out pregnancy as the primary cause of an enlarged uterus or amenorrhea.
- Full Blood Count (FBC) & Iron Studies: To confirm and quantify the severity of anemia caused by heavy bleeding.
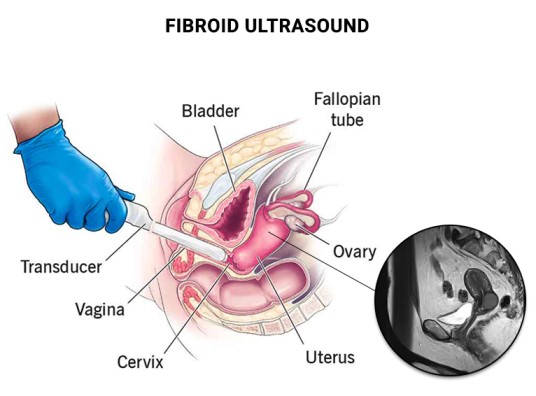
- Pelvic Ultrasound (U/S): The standard, non-invasive imaging test to clearly visualize the uterus and detect the size and number of fibroids.
- Transvaginal Ultrasound (TVUSS): Inserting a small probe into the vagina provides a much clearer, high-resolution view of the pelvic organs, which is especially useful in obese patients.
- Saline Hysterosonography: Injecting sterile saline into the uterus during an ultrasound to sharply outline the cavity and identify hidden submucous fibroids.
- Hysterosalpingogram (HSG): An X-ray procedure using contrast dye to visualize the exact shape of the uterine cavity and ensure the fallopian tubes are open (crucial for infertility workups).
- Hysteroscopy: Passing a thin, lighted camera (hysteroscope) through the vagina and cervix directly into the uterus to visualize and potentially remove submucosal fibroids.
- MRI (Magnetic Resonance Imaging): The most highly accurate tool for mapping out the exact size, location, and vascularity of every single fibroid prior to complex surgeries.
Differential Diagnosis (DDx)
Fibroids are usually easily diagnosed, but the midwife/clinician must clinically exclude other conditions that cause similar presentations:
- Exclude Pregnancy: Always the absolute first step for an enlarged uterus.
- Exclude Other Pelvic Masses: Ovarian Carcinoma, Tubo-ovarian abscesses, Endometriosis, or Adnexa/omentum/bowel that has adhered to the uterus.
- Exclude Other Causes of Uterine Enlargement: Adenomyosis, Generalized Myometrial hypertrophy, Congenital anomalies, or Endometrial Carcinoma.
- Exclude Other Causes of Abnormal Bleeding: Endometrial hyperplasia, Endometrial or tubal Carcinoma, Uterine sarcoma, Polyps, and Dysfunctional Uterine Bleeding (DUB).
⚠️ Attention: Rule Out Malignancy
An endometrial biopsy or Dilation & Curettage (D&C) is strictly essential in the evaluation of any abnormal uterine bleeding to definitively exclude Endometrial Carcinoma before assuming the bleeding is solely from a fibroid.
Management of Uterine Fibroids
Most fibroids are totally asymptomatic and require expectant management (watchful waiting), especially since they shrink naturally after menopause. When treatment is required, the choice depends on: Age, Parity, Size/Location of the fibroids, Desire to preserve the uterus, and the Desire for future pregnancies.
1. Emergency Treatment
- Blood Transfusion: Immediately given to correct life-threatening severe anemia.
- Emergency Surgery (Laparotomy): Indicated immediately for an infected/necrotic myoma, acute torsion (twisting) of a pedicle, or severe intestinal obstruction caused by massive fibroid pressure.
2. Medical Management (Pharmacology)
Medical management does not cure fibroids permanently but controls symptoms and temporarily shrinks them prior to surgery.
- NSAIDs: Nonsteroidal anti-inflammatory drugs (like Ibuprofen) to manage severe pelvic pain and cramping.
- Antifibrinolytic Agents: Tranexamic acid specifically helps to drastically reduce heavy menstrual bleeding (menorrhagia) by preventing blood clots from breaking down too quickly.
- Hormonal Control: Low-dose birth control pills or a Levonorgestrel Intrauterine Device (Mirena coil) effectively limit menstrual blood flow and thin the uterine lining with minimal side effects.
- Haematinics: Aggressive supplementation with Ferrous Sulphate and Folic Acid to rebuild hemoglobin levels in anemic patients.
- GnRH Agonists (Lupron, Synarel): These drugs put the body into a temporary medical menopause by shutting down estrogen and progesterone production from the ovaries. This stops menstruation and significantly shrinks the fibroids.
- Mifepristone: (25-50mg twice weekly) acts as a progesterone receptor inhibitor, effectively reducing fibroid size and stopping bleeding.
- Danazol: A synthetic androgen that interrupts ovulation and shrinks fibroid tissue.
3. Surgical Management
Specific Surgical Criteria
- Open Myomectomy (Laparotomy): The route of absolute choice for large subserous or intramural fibroids measuring greater than 7 cm, multiple fibroids greater than 5 cm, or when direct entry into the uterine cavity is expected.
- Hysteroscopic Myomectomy: The route of choice strictly for removing submucous (SM) fibroids measuring greater than 2 cm.
- Laparoscopic Myomectomy: Mostly done for the subserosal type, removing the mass entirely through a small abdominal keyhole incision.
Advanced Non-Invasive Procedures
- MRGFUS (Magnetic Resonance Guided Focused Ultrasound Surgery): A non-invasive procedure where focused ultrasound waves are converted into intense heat inside the pathology to destroy it, entirely under MRI guidance.
Selection Criteria: Fibroid must be 4 to 10 cm, the woman must have completed her family, and she should be perimenopausal.
- Myomectomy: The surgical removal of the fibroids while leaving the healthy uterus intact.
Indications: Young women who strongly desire future pregnancies, have a few isolated fibroids, but suffer from heavy bleeding or infertility. - Hysterectomy: The complete surgical removal of the entire uterus.
Indications: Women who have completed their families, are approaching menopause, have massive/numerous fibroids that destroy the uterine structure, or if there is any suspicion of malignant (cancerous) changes. - Hysteroscopic Resection: Passing a wire loop through the cervix to shave off and remove submucosal fibroids from inside the cavity without cutting the abdomen.
- Endometrial Ablation: Surgically destroying the entire inner lining of the uterus using heat or freezing to permanently stop heavy bleeding (only for women who do not want more children).
- Uterine Artery Embolization (UAE): A radiologist injects tiny polyvinyl particles into the femoral artery, guiding them to block the specific blood vessels feeding the myoma, causing it to starve and shrink.
- Radiofrequency Ablation: Inserting a needle-like device directly into the fibroid and heating the tissue with radiofrequency energy to destroy it.
Pre and Post-Operative Care for Fibroid Surgery
Whether a patient is undergoing a Myomectomy or a Hysterectomy, meticulous nursing care is required to prevent life-threatening surgical complications.
Pre-Operative Management
- Admission & History: Obtain personal, medical, social, and detailed gynecological history. Conduct a full physical head-to-toe examination specifically ruling out severe anemia, dehydration, and jaundice. Ensure a general assessment by the gynecologist is documented.
- Informed Consent: The surgeon must explain the exact reasons for the operation, the benefits, the risks (including the risk of converting a myomectomy to a full hysterectomy if uncontrollable bleeding occurs), and expected results. Involve the partner where culturally or legally appropriate, and secure written consent.
- Investigations: Ensure all preoperative lab work is back on the file: Urinalysis, Hemoglobin (HB) level, Blood Grouping & Cross-matching (ensure at least 2 units of blood are ready), Abdominal ultrasound, Urea and Electrolytes, INR/PT (clotting profile), and an ECG/ECHO if the patient is older or hypertensive.
- Patient Education & Counseling: Educate the patient about what to expect when waking up (pain, catheters, IV lines). Provide strong reassurance to relieve surgical anxiety.
- Physical Preparation: Ensure the patient fasts from food and drinks (NPO) for at least 8 hours prior. Shave and prep the abdominal/pubic area. Arrange for a wide-bore IV line insertion. Insert a urethral Foley catheter to keep the bladder completely empty and safe from surgical injury. Administer prescribed pre-medications.
- Theatre Transfer: Help the patient change into a clean theatre gown, remove jewelry and dentures, and wheel her to the operating theatre while providing continuous emotional support.
Post-Operative Management
- Reception & Positioning: Receive the patient from the recovery room into a pre-warmed bed. Keep her lying flat (supine for abdominal surgery) with the head turned to one side to prevent aspiration if she vomits.
- Intensive Observation: Take vital signs continuously (every 15 minutes for the first hour, then every 30 minutes until fully stable). Closely monitor BP and pulse for early signs of internal hemorrhage or hypovolemic shock. Check the surgical dressing for active bleeding. Monitor the IV infusion rate and continuous blood transfusions.
- Upon Full Consciousness: Gently welcome the patient, orient her to the ward, and explain that the surgery was successful. Assist with face sponging, provide mouthwash to relieve dry mouth, and change her into a fresh gown.
- Medical Treatment & Pain Relief: Administer strong analgesics precisely as prescribed (e.g., IM Pethidine 100mg every 8 hours for the first 24 hours, then step down to oral Paracetamol/NSAIDs). Administer broad-spectrum IV antibiotics (e.g., Ampicillin/Gentamicin) to prevent pelvic sepsis. Continue Haematinics and Vitamin C to aid rapid wound healing.
- Wound Care: Monitor the abdominal wound closely. If minor strike-through bleeding occurs, do not remove the dressing; simply reinforce it with a fresh bandage on top and notify the surgeon.
- Nursing & Rehabilitative Care: Maintain strict hygiene (bed baths, catheter care). Once bowel sounds return and the doctor permits, start sips of water and progress to a soft diet. Encourage deep chest breathing and early leg exercises while in bed to prevent Deep Vein Thrombosis (DVT) and chest infections. Assist with early ambulation.
Specific Vaginal Surgery Management (If applicable)
- If a vaginal pack was inserted to control hemorrhage, inspect it frequently for soakage.
- Once the pack is removed (usually after 24 hours), apply a sterile vulval pad. Swab and clean the vulva at least every 8 hours using aseptic technique to prevent ascending infections.
🧠 Discharge Advice (Crucial for Myomectomy)
For Myomectomy Patients: The uterine wall has been cut and scarred. Advise the mother to strictly avoid conception for at least 2 years to allow the uterine scar to achieve maximum strength. When she does conceive, she must deliver via Elective Cesarean Section to prevent a catastrophic uterine rupture during labour.
For Hysterectomy Patients: Provide deep psychological counseling. Assure her she will no longer have periods and cannot conceive, but her sexual function will remain intact once healed. Recommend abstaining from sexual intercourse for 6 weeks.
Complications of Uterine Fibroids
General Gynecological Complications
- Severe Menorrhagia: Leading to chronic, debilitating iron-deficiency anemia.
- Infertility: Due to blocked tubes or a distorted endometrial cavity preventing embryo implantation.
- Torsion: A pedunculated fibroid twisting on its stalk, causing acute ischemic pain and gangrene.
- Urinary Tract Diseases: Chronic retention of urine leading to repeated severe urinary tract infections (UTIs) and hydronephrosis (kidney swelling) due to ureter compression.
Complications During Pregnancy and Labour
If a woman with significant fibroids conceives, the pregnancy is automatically classified as High Risk due to the following massive threats:
- Antepartum Hemorrhage (APH): The presence of fibroids heavily increases the risk of Placenta Previa and Placental Abruption.
- Abortion/Miscarriage: The distorted cavity lacks enough healthy blood supply to sustain the early placenta.
- Fetal Growth Restriction (FGR): The fibroids steal the blood supply away from the growing baby, leading to a small, undernourished fetus.
- Malpresentation: Large fibroids block the baby from turning properly, leading to Breech or Transverse lies.
- Labor Dystocia & Obstruction: A cervical or lower segment fibroid acts as a literal physical roadblock, causing completely Obstructed Labour.
- Premature Labor: The uterus becomes overstretched too early by the combined bulk of the baby and the fibroids.
- Uterine Inertia & PPH: The fibroid-riddled myometrium loses its ability to contract effectively. This leads to weak labour (inertia) and massive Postpartum Hemorrhage (PPH) because the uterus cannot clamp down on the bleeding blood vessels.
- Subinvolution: During the puerperium, the fibroid prevents the uterus from shrinking back to normal size, causing prolonged, heavy lochia.
Clinical Nursing Care Plan: Uterine Fibroids
Clinical Scenario: Mrs. A.O., a 44-year-old teacher, is admitted for a scheduled total abdominal hysterectomy due to symptomatic fibroids. Complaints: Menorrhagia (bleeding 8-10 days, soaking pad/super tampon hourly), pelvic pain/pressure (5/10), and severe fatigue. Pre-op Hb: 9.8 g/dL. She feels "drained" and is highly anxious about surgery and loss of fertility.
| Assessment & Nursing Diagnosis | Goals / Expected Outcomes | Nursing Interventions & Rationale | Evaluation |
|---|---|---|---|
|
Subjective: Constant pelvic pain/pressure 5/10. "Heavy ball in stomach." Objective: Confirmed fibroids, palpable firm enlarged uterus, guarding lower abdomen. Diagnosis: Chronic Pain related to pressure from enlarged fibroids on pelvic organs/nerves. |
- Report pain decrease to manageable level (< 3/10). - Demonstrate two non-pharmacological relief techniques. - Rest comfortably. |
Interventions: 1. Conduct comprehensive pain assessment. 2. Administer prescribed NSAIDs on a scheduled basis. 3. Teach non-pharmacological comfort (heating pad, guided imagery). 4. Position in semi-Fowler's or side-lying with pillows. Rationale: Scheduled dosing provides consistent analgesia. Positioning alleviates direct fibroid pressure on structures. |
Goals Met. Patient reports pain is 2/10 after scheduled ibuprofen and heating pad. Resting comfortably in semi-Fowler's. |
|
Subjective: "Drained all the time, no energy." Reports menorrhagia. Objective: Pale conjunctiva, Hb 9.8 g/dL, lethargic, mild tachycardia on exertion. Diagnosis: Excessive Fatigue burden related to chronic blood loss and anemia. |
- Identify relationship between heavy bleeding, anemia, and fatigue. - Participate in energy conservation. - Verbalize anemia management plan. |
Interventions: 1. Cluster nursing activities; schedule rest periods. 2. Administer iron supplements with Vitamin C. 3. Educate on fatigue causes linking to blood loss. 4. Provide an iron-rich diet (lean meat, spinach). Rationale: Vitamin C heavily enhances iron absorption. Energy conservation prevents exhaustion while maintaining dignity. |
Goals Met. Patient explains, "My heavy periods made my blood count low, which is why I'm tired." Taking iron actively. |
|
Subjective: "Worried about surgery. Feels strange not having a uterus." Objective: Restless, anxious expression, increased HR/BP when discussing surgery. Diagnosis: Excessive Anxiety related to impending major surgery, body image changes, and loss of fertility. |
- Verbalize specific fears. - Report noticeable decrease in anxiety. - Demonstrate effective coping mechanisms (deep breathing). |
Interventions: 1. Establish a trusting relationship to express feelings. 2. Provide clear, factual pre/post-op routine info. 3. Teach relaxation (mindfulness, calming music). 4. Acknowledge and validate grief over end of fertility. Rationale: Validation normalizes emotional response. Factual knowledge dispels myths and reduces fear of the unknown. |
Goals Met. Patient reports feeling "less on edge" after talking through fears. Listening to music to relax. |
|
Subjective: Soaking pad and tampon hourly. Objective: Scheduled for total abdominal hysterectomy. Pre-existing anemia. Diagnosis: Risk for Bleeding related to underlying condition and impending surgery. |
- Remain hemodynamically stable. - Pre-op prep for blood loss completed. - Verbalize post-op signs of excessive bleeding to report. |
Interventions: 1. Ensure current CBC, blood type, and screen are on chart. 2. Monitor vitals for hypotension/tachycardia. 3. Educate to report soaking >1 pad/hour post-op. 4. Ensure surgical consent (incl. blood transfusion) is signed. 5. Assess/stop anticoagulant use (NSAIDs/fish oil). Rationale: Type/screen ensures blood is readily available. Stopping NSAIDs prevents coagulation failure during surgery. |
Goals Met. Labs complete, consent signed. Patient states two signs of post-op bleeding to report. Hemodynamically stable. |
References
- 1. Myles Textbook for Midwives (Latest Edition) - Anatomy and Physiology of the Female Reproductive System.
- 2. DC Dutta's Textbook of Gynecology - Benign Lesions of the Uterus.
- 3. UNMEB Curriculum for Diploma in Midwifery Extension Program - Gynaecology & Reproductive Health (DME 112).
- 4. Clinical Guidelines for Obstetrics and Gynaecology (Ministry of Health, Uganda).

Some sub topics cannot be opened
Well done senior notes are easy to understand.
Work is good. However some sub topics can not open like starting from congenital abnormalities to ovarian cyst!