
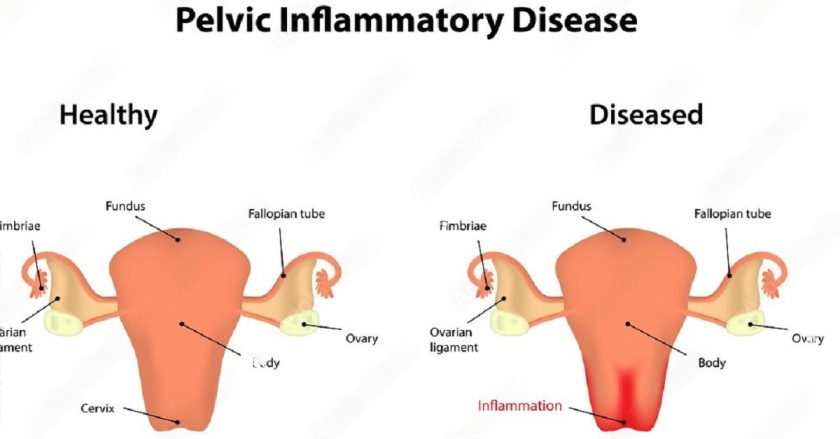
Pelvic Inflammatory Diseases (PID)
Pelvic Inflammatory Diseases (PID) refer to a spectrum of severe, acute, or chronic infections that ascend and affect the upper female genital tract and its surrounding structures.
These affected pelvic organs and structures primarily include:
- The Cervix (Cervicitis)
- The Endometrium (Endometritis)
- The Fallopian Tubes (Salpingitis)
- The Ovaries (Oophoritis)
- The Pelvic Peritoneum and Pelvic Vascular System
PID is a major cause of gynecological morbidity, contributing heavily to female infertility, chronic pelvic pain, and ectopic pregnancies.
Causes and Causative Organisms of PID
PID is rarely caused by a single mechanism; it is usually a polymicrobial infection. The infection reaches the sterile upper genital tract through three primary routes of spread:
- 1. Ascending Infections: This is the most common route. It occurs when pathogenic bacteria from the vagina or cervix travel upwards through the endocervical canal into the normally sterile reproductive organs (uterus, fallopian tubes, and ovaries).
- 2. Haematogenous Infections: Infections that are spread systemically through the bloodstream to reach the pelvic organs (e.g., Tuberculosis).
- 3. Direct Spread: Infection spreading from infected neighboring or adjacent organs. For example, a ruptured or highly infected appendix (appendicitis) can directly spill purulent material into the pelvic region, infecting the fallopian tubes.
Specific Causative Organisms
PID is often polymicrobial, involving both aerobic and anaerobic bacteria. The most common culprits include:
- Neisseria gonorrhoeae: A primary sexually transmitted pathogen responsible for severe acute PID.
- Chlamydia trachomatis: Another major sexually transmitted pathogen, often causing silent or subclinical but highly destructive PID.
- Haemophilus influenzae
- Escherichia coli (E. coli): Common in obstetric PID or when bowel flora cross-contaminates the vagina.
- Anaerobes: Organisms associated with bacterial vaginosis (e.g., *Gardnerella vaginalis*).
Risk Factors for Developing PID
Certain behavioral, medical, and obstetric factors highly increase a woman's vulnerability to developing Pelvic Inflammatory Disease. These include:
- History of STIs: Previous or current untreated sexually transmitted infections, especially Gonorrhea and Chlamydia.
- Bacterial Vaginosis (BV): An overgrowth of harmful bacteria causing an imbalance in normal, protective vaginal flora (Lactobacilli).
- Sexual Practices: Having multiple sexual partners or a partner who has multiple partners, increasing exposure to pathogens.
- Douching: This practice vigorously washes away protective vaginal mucus and flora, and can actively push existing lower tract bacteria up into the uterus.
- Previous History of PID: One episode of PID heavily damages protective mucosal barriers, drastically increasing the risk of recurrence.
- Use of Intrauterine Devices (IUDs): The risk is slightly elevated immediately after insertion if pre-existing cervical infections are pushed into the uterus.
- Surgical/Gynecological Procedures: Invasive procedures like Dilation and Curettage (D&C), manual vacuum aspiration, or hysteroscopy can introduce bacteria.
- Obstetric Causes: Infections following abortion, ectopic rupture, or puerperal sepsis (postpartum infections).
Pathophysiology of PID
The disease process of PID is highly destructive to the delicate reproductive tissues. It typically follows this pattern:
- The infection typically begins localized in the vagina and cervix (often asymptomatic or presenting as mild cervicitis).
- The bacteria then actively ascend through the endocervical canal to reach the Fallopian tubes and ovaries. During menstruation, the endocervical canal naturally dilates slightly and the protective cervical mucus plug is lost, facilitating the easy entry of bacteria into the uterus.
- Once inside the highly vascular reproductive tracts, the bacteria rapidly multiply. The body's immune response triggers massive inflammation.
- This inflammation destroys the tiny, hair-like cilia inside the fallopian tubes, causing purulent exudate (pus) to build up.
- The infection can then easily spill out of the open ends (fimbriae) of the fallopian tubes, spreading further to the ovaries, the pelvic peritoneum, and even other abdominal organs, causing severe peritonitis.
Clinical Manifestations (Signs and Symptoms)
The clinical presentation of PID can vary from mild, vague discomfort to an acute, life-threatening acute abdomen. Diagnosis relies heavily on detailed history-taking and physical examination.
1. On History Taking (What the Patient Reports)
- Severe Lower Abdominal Pain: Approximately 70% of individuals with PID experience intense, continuous pain in the lower abdomen. It can be localized (one side) or diffuse (spread out). It heavily worsens during movement, walking, or sexual activity (dyspareunia).
- Acute Fever: Around 40% of PID cases present with a high fever (often >38°C) accompanied by chills, responding to the massive internal infection.
- Purulent Vaginal Discharge: About 90% of PID patients complain of a heavy, purulent (pus-like) vaginal discharge. It is often thick, yellowish or greenish, and foul-smelling.
- Menstrual Changes: Severe inflammation disrupts normal hormonal and uterine function leading to:
- Dysmenorrhea: Extremely painful menstrual periods.
- Menorrhagia: Heavy or abnormally prolonged bleeding.
- Oligomenorrhea: Infrequent, irregular, or scanty periods.
2. On Physical Examination (What the Midwife/Doctor Finds)
- Signs of Inflammation: The pelvic region may feel unusually warm, swollen, and look reddened externally.
- Peritoneal Signs: Abdominal palpation reveals peritonitis signs: Guarding (involuntary tensing of abdominal muscles to protect inflamed organs), Abdominal distension, and Rebound tenderness (sharp pain felt when the examiner's pressing hand is quickly released).
- Vaginal Examination (Speculum & Bimanual):
- Vaginal Changes: The vaginal walls appear red, highly inflamed, and dry due to ongoing local irritation.
- Purulent Discharge: Pus is visibly seen escaping from the cervical os.
- Cervical Excitation (Chandelier Sign): Extreme pain when the cervix is gently moved side to side during a bimanual exam.
- Tender Fornices: Palpation of the vaginal fornices reveals extreme tenderness and possibly a swollen mass, indicating pyosalpinx (accumulation of pus in the Fallopian tubes).
Specific Pelvic Infections Breakdown
PID is an umbrella term. Depending on exactly where the infection settles, it is medically divided into the following specific inflammatory conditions:
Condition Definition Specific Signs & Symptoms Cervicitis Inflammation of the cervix (the lower part of the uterus opening into the vagina). Often caused by Chlamydia/Gonorrhea. - Red, swollen cervix.
- Cervical friability: Slight bleeding on intercourse or contact.
- Itching/burning sensation in the vagina.
- Watery, yellowish, or greenish abnormal discharge.
Endometritis Inflammation of the endometrium (the inner lining of the uterus). Often occurs postpartum, post-abortion, or post-IUD insertion. - Enlargement of the uterus: Feels boggy, tender, and larger than normal.
- Foul-smelling, offensive lochia/discharge.
- Lower abdominal pain and high fever.
Salpingitis Inflammation of one or both fallopian tubes. It is a highly destructive complication causing tubal blockage. - Severe lower abdominal or lower back pain.
- Dyspareunia: Deep pain during sexual intercourse.
- Risk of forming a pus-filled tube (pyosalpinx).
Oophoritis Inflammation of one or both ovaries. Often occurs in conjunction with salpingitis (Salpingo-oophoritis). - Deep pelvic, abdominal, and back pain.
- Dyspareunia.
- Palpable, highly tender adnexal mass.
Hospital Management of PID
Because PID can permanently damage a woman's reproductive system, aggressive, immediate, and comprehensive management is required.
1. Main Aims of Management
- To strictly prevent permanent complications (like infertility and ectopic pregnancy).
- To quickly relieve the intense pain.
- To completely eradicate the infection and prevent the disease from spreading to the peritoneum or systemic bloodstream.
2. Nursing & Supportive Care
- Admission & Position: Admit the patient to a clean, well-ventilated gynecological ward for strict, complete bed rest. Place the patient in a Semi-Fowler’s position (propped up). Gravity assists in draining the purulent discharge downwards and prevents the pus from flowing upwards into the abdominal cavity (preventing generalized peritonitis).
- Hydration: The patient is often febrile and dehydrated. Start an I.V. line immediately and administer intravenous fluids (like Normal Saline or Ringer's Lactate). Encourage high oral fluid intake if she can tolerate it without vomiting.
- Histories & Examination: Take exhaustive medical and sexual histories. Conduct a comprehensive general and abdominal examination.
- Continuous Observations: Monitor vital signs strictly (Temperature, Pulse, Respiration, Blood Pressure) every 4 hours. Daily, observe and accurately record the color, specific amount, and smell of the vaginal discharge on a fluid chart.
- Diet & Elimination: Advise a highly nutritious, easily digestible diet. Provide a bedpan or urinal to maintain bed rest. Observe the urine; disinfect urine and feces with a strong hypochlorite solution (like JIK) before disposal to prevent cross-infection.
- Hygiene & Exercise: Perform bed-making daily, removing wrinkles to prevent bedsores. Once the fever breaks and pain reduces, encourage light physical exercise (like walking around the ward) to prevent DVT.
- Care of Mind (Psychotherapy): Severe pain and fears of infertility cause high anxiety. Reassure the patient and her relatives constantly. Provide diversional therapies like newspapers, TV, or radios.
3. Diagnostic Investigations
Do not delay initial treatment waiting for results, but perform these urgently:
- High Vaginal Swab (HVS) / Endocervical Swab: Sent for Culture and Sensitivity (C&S) to exactly identify the causative bacteria (e.g., Gonorrhea).
- Urinalysis: For C&S to rule out a concurrent severe Urinary Tract Infection (UTI).
- Blood Tests: A blood culture for C&S to check for a hematogenous (bloodstream) source or septicemia. A malaria blood slide (BS) to rule out malaria as a cause of the high fever. Complete Blood Count (CBC) to check for highly elevated White Blood Cells (Leukocytosis).
- Ultrasound Scan: A pelvic scan is critical to rule out other severe causes of acute abdominal pain (e.g., ruptured ectopic pregnancy, acute appendicitis, or the presence of a massive Tubo-Ovarian Abscess).
4. Medical Treatment (Pharmacology)
Treatment is started immediately using powerful broad-spectrum antibiotics before laboratory results return, covering both aerobic and anaerobic bacteria.
- Initial I.V. Antibiotic Regimens:
- Ceftriaxone 2g daily IV for 5 days.
- Chloramphenicol 2g stat, then 1g 6-hourly for 5 days.
- Gentamicin 160mg Once Daily (OD) for 5 days.
- Metronidazole 500mg I.V. 8-hourly (TDS) for strict anaerobic coverage.
- Oral Step-Down Therapy: If the fever subsides and discharge drastically reduces, switch to oral antibiotics based on sensitivity results. Common choices include Azithromycin (1g single dose for Chlamydia), Doxycycline (100mg BD for 14 days), Ciprofloxacin, or Tetracycline.
- Analgesics: Severe pain requires powerful relief. Administer strong NSAIDs like Diclofenac or Ibuprofen to reduce both pain and local inflammation. In extremely severe cases, short-term narcotics (e.g., Pethidine) may be required. Paracetamol is used to control fever.
⚠️ Attention: Severe Complications of PID
If PID is left untreated, inadequately treated, or if the patient presents too late, the irreversible destruction of pelvic tissues leads to life-altering complications:
- Infertility: Severe inflammation leaves thick scar tissue blocking the fallopian tubes, preventing the sperm from reaching the egg.
- Ectopic Pregnancy: The damaged, narrowed tubes may allow sperm up, but trap the larger fertilized embryo, causing it to grow and dangerously rupture the fallopian tube.
- Pelvic Abscess & Tubo-Ovarian Mass: Massive collections of walled-off pus (abscesses) forming dangerous masses involving the tubes and ovaries.
- Chronic Pelvic Pain & Adhesions: Thick scar tissue binds the pelvic organs and intestines together like glue, causing permanent, agonizing daily pain.
- Intestinal Obstruction & Peritonitis: Severe infection spills into the abdominal cavity, paralyzing or blocking the bowels.
Advice on Discharge
A comprehensive counseling session must be held before the patient goes home to prevent recurrence:
- Medication Compliance: Strictly complete the entire 14-day course of oral antibiotics, even if the pain has completely stopped.
- Partner Treatment: Emphasize that all recent sexual partners MUST be tested and treated simultaneously to prevent the "ping-pong" re-infection cycle.
- Safe Sex Practices: Strongly advise a reduction in multiple sexual partners. Advocate for the strict, consistent use of barrier methods (condoms).
- Contraception Review: Advise avoiding Intrauterine Contraceptive Devices (IUDs) if she is at high risk for STIs. Discuss safer alternative methods.
- Hygiene: Educate on proper perineal hygiene (wiping front to back) and strictly forbid vaginal douching.
- Follow-up: Instruct the patient to return to the clinic immediately for review if she experiences a relapse of pain, abnormal discharges, itching, or fever.
💡 Quick Practice Check
Question: Why is a patient admitted with severe acute PID placed specifically in a Semi-Fowler’s (propped up) position in bed?
Answer: To utilize gravity to help drain the toxic, purulent discharge downwards and out through the vagina, preventing the pus from tracking upwards and spilling into the abdominal cavity, which would cause a deadly generalized peritonitis.

Endometritis
Endometritis is a specific inflammatory condition characterized by the severe inflammation and infection of the endometrium (the innermost mucosal lining of the uterus).
It can present as an acute infection (sudden and severe) or a chronic condition (long-lasting, often silent). It is one of the most common precursors to widespread Pelvic Inflammatory Disease (PID) if the bacteria are allowed to ascend further into the fallopian tubes.
Causes and Major Risk Factors
Endometritis is primarily caused by an ascending bacterial infection from the lower genital tract (vagina or cervix). The highly vascular, nutrient-rich lining of the uterus provides a perfect environment for rapid bacterial multiplication once the protective cervical barrier is breached.
The condition is most commonly triggered by major obstetric or surgical events that introduce bacteria directly into the uterine cavity:
- Postpartum (Childbirth): The most common cause. After delivery, the raw, open placental site acts as a massive wound. If bacteria enter during prolonged labour, frequent vaginal examinations, or unhygienic delivery practices, puerperal endometritis develops rapidly.
- Post-Abortion: Induced or spontaneous abortions (miscarriages), especially if retained products of conception (tissue) are left behind in the uterus, provide a breeding ground for bacteria.
- IUD Insertion: The physical insertion of an Intrauterine Contraceptive Device (IUD) can accidentally push pre-existing cervical bacteria (like Chlamydia or Gonorrhea) up into the sterile endometrium.
- Gynecological Procedures: Invasive procedures such as Dilation and Curettage (D&C), hysteroscopy, or endometrial biopsies.
Clinical Manifestations (Signs and Symptoms)
A mother or patient presenting with endometritis will typically exhibit a combination of localized pelvic symptoms and systemic signs of infection. The midwife must carefully assess for the following:
- Acute Fever and Chills: The patient will often present with a suddenly elevated body temperature (typically above 38.0°C or 100.4°F) accompanied by chills and tachycardia (fast heart rate). This is the body's aggressive systemic response to the bacterial infection inside the uterus.
- Severe Lower Abdominal Pain: A hallmark symptom. The patient will complain of continuous, deep, dull, or cramping pain and extreme discomfort in the lower abdomen/pelvic region due to the severe swelling of the uterine lining.
- Abnormal Vaginal Discharge: The infection produces heavy, purulent (pus-filled) vaginal discharge. In postpartum women, this manifests as highly offensive, foul-smelling lochia that may appear yellowish, greenish, or dark brown and prolonged.
- Enlargement of the Uterus (Subinvolution): Upon abdominal palpation or bimanual examination, the uterus will feel extremely tender, "boggy" (soft instead of firm), and larger than expected. The severe inflammation prevents the uterine muscles from effectively contracting and shrinking back to their normal size.
- General Malaise: The patient will look visibly ill, fatigued, and may experience anorexia (loss of appetite), nausea, or headaches due to the circulating bacterial toxins.
⚠️ Attention: The Danger of Untreated Endometritis
Endometritis is a medical emergency. If the infection is not aggressively treated with strong intravenous broad-spectrum antibiotics, the bacteria will rapidly ascend out of the uterus and destroy the upper reproductive organs, leading to permanent, irreversible complications.
Severe Complications of Untreated Endometritis
Poorly managed or delayed treatment of endometritis sets off a chain reaction of destructive pelvic inflammatory diseases. The direct complications include:
- Salpingitis: The infection spreads directly from the uterine lining into the fallopian tubes, causing severe inflammation and filling the tubes with pus (pyosalpinx).
- Pelvic Abscess & Tubo-Ovarian Mass: Massive, dangerous pockets of pus form in the pelvic cavity, wrapping around the fallopian tubes and ovaries, often requiring emergency surgery to drain.
- Infertility: The intense inflammation leaves behind thick, fibrous scar tissue that permanently blocks or damages the fallopian tubes, preventing sperm and egg from meeting.
- Ectopic Pregnancy: Because the delicate inner hairs (cilia) of the fallopian tubes are destroyed by the infection, a fertilized egg may get stuck in the tube instead of reaching the uterus, leading to a life-threatening ruptured ectopic pregnancy.
- Chronic Pelvic Pain & Adhesions: Severe scarring causes the pelvic organs (uterus, tubes, ovaries, and bowels) to stick together unnaturally, resulting in debilitating, constant pain that lasts for years.
- Peritonitis: The infection completely spills out of the reproductive tract and deeply infects the entire lining of the abdominal cavity, a deadly condition.
- Intestinal Obstruction: As pelvic adhesions and scar tissue form, they can wrap around and strangle the intestines, causing a partial or complete blockage of the bowels.
💡 Quick Practice Check
Question: A mother who delivered a baby 4 days ago presents to the clinic with a high fever, a soft/boggy uterus that is larger than expected, and highly offensive, foul-smelling lochia. What specific condition must the midwife suspect immediately?
Answer: Puerperal Endometritis. The combination of fever, subinvolution (boggy, enlarged uterus), and foul-smelling discharge in the postpartum period are the classic triad of this dangerous uterine infection.
Endometriosis
Endometriosis is a chronic, often painful gynecological condition where tissue that behaves exactly like the lining of the uterus (the endometrium) grows outside the uterine cavity.
Unlike Endometritis (which is an infection/inflammation of the inside lining), Endometriosis involves stray endometrial tissue implanting on organs such as the ovaries, fallopian tubes, the pelvic peritoneum, the Pouch of Douglas, and sometimes the bowel or bladder.
Because this misplaced tissue responds to monthly ovarian hormones just like the normal uterine lining, it builds up, breaks down, and bleeds every menstrual cycle. However, because this blood has no way to exit the body, it becomes trapped, leading to severe inflammation, excruciating pain, scar tissue, and infertility.
Causes and Theories of Origin
The exact, definitive cause of endometriosis remains a medical mystery. However, several highly researched scientific theories explain how this tissue escapes the uterus:
- Retrograde Menstruation (Sampson’s Theory): This is the most widely accepted theory. It suggests that during menstruation, some of the menstrual blood containing live endometrial cells flows backwards through the fallopian tubes and spills into the pelvic cavity, instead of leaving the body through the vagina. These stray cells then stick to the pelvic walls and organs, where they grow and thicken.
- Cellular Metaplasia: This theory suggests that cells in the abdomen or pelvis retain their embryonic ability to transform (metaplasia) into endometrial cells under the influence of hormones or immune factors.
- Lymphatic and Vascular Spread: Just like cancer cells, endometrial cells may travel through the blood vessels or the lymphatic system to reach distant parts of the body (which explains rare cases of endometriosis found in the lungs or brain).
- Immune System Dysfunction: A normal immune system should recognize and destroy endometrial-like tissue growing outside the uterus. In women with endometriosis, the immune system fails to seek and destroy these rogue cells.
- Surgical Scar Implantation: After surgeries involving the uterus, such as a Cesarean section (C-section) or a myomectomy, endometrial cells can accidentally attach to the surgical incision site (e.g., the abdominal wall scar).
Clinical Manifestations (Signs and Symptoms)
The primary symptom of endometriosis is pelvic pain, often specifically tied to the menstrual cycle. The severity of the pain does not always correlate with the extent of the disease (some women have severe disease but little pain, and vice versa).
- Severe Dysmenorrhea: Excruciating pelvic pain and cramping that begins before the menstrual period and lasts several days into it. It is often described as feeling far worse than "normal" period cramps.
- Dyspareunia: Deep pelvic pain during or immediately after sexual intercourse. The thrusting motion hits the tender, inflamed endometrial nodules tethered behind the uterus or in the vaginal fornices.
- Chronic Pelvic Pain: A continuous, heavy, dull ache in the lower abdomen, lower back, and pelvis that happens even when not menstruating.
- Dyschezia and Dysuria: Intense pain during defecation (passing stool) or urination, particularly during the menstrual period. This occurs when endometrial tissue implants on the bowel or bladder.
- Menorrhagia and Menometrorrhagia: Experiencing excessively heavy menstrual periods or bleeding irregularly between periods.
- Infertility: Endometriosis is diagnosed in up to 50% of women seeking treatment for infertility. The thick scar tissue (adhesions) distorts the pelvic anatomy, blocking the fallopian tubes and preventing the egg and sperm from uniting.
⚠️ Attention: The "Chocolate Cyst"
When endometrial tissue implants deeply into an ovary, it bleeds into itself every month. Over time, this old, trapped, oxidized blood turns thick and dark brown, forming an Endometrioma, classically referred to in gynecology as a "Chocolate Cyst." If a chocolate cyst ruptures, it causes an acute, surgical abdominal emergency.
Diagnosis of Endometriosis
Because the symptoms heavily mimic other pelvic diseases (like PID or Ovarian Cysts), a definitive diagnosis requires specialized investigations:
- Detailed Pelvic Examination: The healthcare provider may feel cysts on the reproductive organs or thick scars behind the uterus.
- Transvaginal Ultrasound (TVUS): Highly effective for identifying specific endometrial cysts (endometriomas) on the ovaries, though it may miss smaller, flat implants.
- Magnetic Resonance Imaging (MRI): Gives a much more detailed image to map out the exact locations and depths of the endometrial implants prior to surgery.
- Diagnostic Laparoscopy (The Gold Standard): A tiny camera is inserted through a small abdominal incision. This is the only way to 100% definitively diagnose endometriosis. The surgeon can directly visualize the classic "powder-burn" lesions, take a biopsy for histology, and remove the implants simultaneously.
Management and Treatment
There is currently no absolute cure for endometriosis. Treatment is highly individualized based on the severity of symptoms, the extent of the disease, and whether the woman desires to have children in the future.
1. Medical / Pharmacological Management
The goal is to relieve pain and suppress the menstrual cycle, effectively starving the misplaced tissue of the hormones it needs to bleed and grow.
- Analgesics: Non-steroidal anti-inflammatory drugs (NSAIDs) like Ibuprofen or Diclofenac are used aggressively to reduce inflammation and severe cramping.
- Hormonal Contraceptives: Combined oral contraceptive pills (COCs), patches, or vaginal rings are used continuously to stop the hormonal fluctuations, thereby reducing or entirely stopping the bleeding and pain.
- Progestin Therapy: Progestin-only pills, contraceptive implants, or the Mirena IUD halt the menstrual periods and prevent the growth of endometrial implants.
- GnRH Agonists (e.g., Danazol, Zoladex): These powerful drugs block the production of ovarian-stimulating hormones, causing a temporary "medical menopause." This stops menstruation entirely, forcing the endometriosis to drastically shrink.
2. Surgical Management
- Conservative Surgery (Laparoscopy): For women trying to get pregnant or suffering severe pain. The surgeon carefully excises (cuts out) or burns away (ablates) the endometrial lesions and scar tissue while leaving the healthy uterus and ovaries perfectly intact.
- Definitive Surgery (Hysterectomy): Used only as a last resort for women who have severe, uncontrollable pain and do not wish to have any more children. It involves the total removal of the uterus (Total Abdominal Hysterectomy), and frequently the removal of both ovaries and fallopian tubes (Bilateral Salpingo-Oophorectomy) to permanently stop all hormone production.
3. Nursing Care and Psychotherapy
- Provide extensive emotional support. Endometriosis causes immense psychological stress, depression, and anxiety due to chronic pain, dyspareunia (which damages relationships), and the devastating fear of infertility.
- Educate the mother extensively on her medication compliance, especially the side effects of hormone therapies (like weight gain or menopausal flashes from GnRH agonists).
- Encourage attendance at specialized fertility or chronic pain support groups.
💡 Quick Practice Check
Question: A 28-year-old woman is admitted to the gynecology ward complaining of severe, incapacitating pelvic pain exactly three days before her period starts, deep pain during sexual intercourse, and inability to conceive for 3 years. Her ultrasound reveals a large "chocolate cyst" on her left ovary. What is the most likely diagnosis?
Answer: Endometriosis. The classic triad of severe dysmenorrhea, dyspareunia, and infertility, combined with an endometrioma (chocolate cyst) on the ovary, points definitively to endometriosis.
References
- Ministry of Health (MOH) Uganda - National Clinical Guidelines for the Management of Common Conditions.
- Berek, J. S. (Ed.). Berek & Novak's Gynecology. Wolters Kluwer.
- Syllabus guidelines for Diploma in Midwifery Extension Program, Uganda Nurses and Midwives Council (UNMEB).

Special thnxs 2 e initiation, bt some notes aren’t assessed n’t evn opening.
Thanks for helping , but some notes are not opening and seen THANKS 🙏