
Ectopic Pregnancy
1. Definition and Causes
Normally, a fertilized egg travels down the fallopian tube and embeds safely inside the thick lining of the uterus. In an ectopic pregnancy, the fertilized ovum embeds outside the uterine cavity.
Causes and Risk Factors
Any condition that slows down or prevents the fertilized egg from moving smoothly down the fallopian tube can cause an ectopic pregnancy.
- Pelvic Inflammatory Disease (PID): Infections like salpingitis (inflammation of the tubes) destroy the tiny hair-like structures (cilia) inside the tube. PID also forms sticky scar tissue (adhesions) that stop the normal wave-like squeezing motions (peristalsis) of the tubes.
- Fallopian Tube Damage & Congenital Issues: Previous infections or surgeries can leave behind thick scars. Some women are also born with abnormally long tubes that easily kink (bend), or congenitally narrow tubes, making it hard for the egg to pass.
- Previous Ectopic Pregnancy: A woman who has already suffered one ectopic pregnancy is at a much higher risk of having another one because the underlying tube damage is usually still present.
- Endometriosis: This is the abnormal growth of the uterine lining (endometrium) in places outside the uterus. The fertilized egg may accidentally implant on this misplaced tissue.
- Repeated Induced Abortions: Multiple scraping procedures can introduce infections or cause scarring that damages the reproductive pathways.
- Tubal Surgery: Surgical operations on the fallopian tubes (like tying them or attempting to unblock them) create scars inside (intraluminal) or outside (extraluminal) the tubes.
- Intrauterine Devices (IUDs): While IUDs are great at preventing normal pregnancies inside the uterus, if a pregnancy *does* accidentally happen with an IUD in place, it is highly likely to be ectopic because the device blocks the normal implantation site.
- Tumors: Large growths, like fibroids or ovarian cysts, can press hard against the outside of the fallopian tube, causing a partial or complete physical blockage.
- Hormonal Factors: Imbalances in hormones can slow down the movement of the egg and affect how quickly it implants.
- Reproductive System Abnormalities: Being born with a misshapen uterus (like a bicornuate uterus) or abnormally placed tubes.
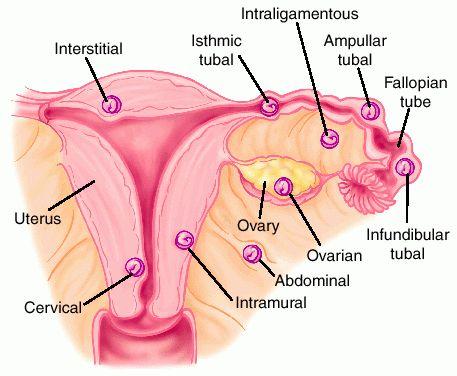
2. Sites of Ectopic Pregnancy
An ectopic pregnancy can happen in several places, but the Fallopian Tubes are by far the most common site (accounting for about 95% of cases). Other rare sites include the broad ligament, the ovary, the cervix, and the intraperitoneal abdominal cavity.
Specific Sites for Tubal Pregnancy
- Ampulla (Most Common): The widest part of the fallopian tube where fertilization usually occurs. The egg often gets stuck here.
- Isthmus (Most Dangerous): The narrowest part of the tube. Because it is so small and tight, a growing pregnancy here will cause the tube to burst (rupture) very early, sometimes even before the mother misses her period or realizes she is pregnant.
- Fimbriated End (Infundibulum): The finger-like ends of the tube (rare site).
- Interstitial Part: The section of the tube that crosses through the thick uterine wall (rare but causes massive bleeding if ruptured).
3. Possible Outcomes of a Tubal Pregnancy
If the egg implants in the tube, the pregnancy cannot last to term. One of four things will eventually happen:
| Outcome | Clinical Description |
|---|---|
| 1. Tubal Mole | The fertilized egg (zygote) dies quietly. It is retained inside the fallopian tube, completely surrounded by a thick blood clot. This may result in a slow-leaking, chronic ectopic pregnancy with mild, lingering pain. |
| 2. Tubal Abortion | The zygote completely detaches from the wall of the fallopian tube and is pushed out (expelled) through the open fimbriated end into the abdomen. It may die and be absorbed, or very rarely, it can stick to abdominal organs and become an abdominal pregnancy. |
| 3. Tubal Rupture | The growing baby quickly becomes too large for the tiny tube. The tube violently bursts open, tearing major blood vessels. This causes massive internal bleeding straight into the abdominal cavity, leading to sudden, severe hypovolemic shock. |
| 4. Tubal Erosion | The aggressive cells of the growing zygote slowly eat through (erode) the wall of the fallopian tube, causing a steady leakage of blood into the abdominal cavity. |
⚠️ Clinical Emergency: Tubal Rupture
A ruptured ectopic pregnancy is a top-tier obstetric emergency. The mother can bleed to death internally in a matter of hours. Always suspect an ectopic pregnancy in any woman of childbearing age presenting with abdominal pain and fainting, even if she claims she is not pregnant.
4. Signs and Symptoms (Focusing on Tubal Rupture)
On History Taking
- Amenorrhea: A clear history of missing her periods for 6 to 10 weeks.
- General Danger Signs: The patient heavily complains of feeling faint, extreme dizziness, severe thirst (a classic sign of internal bleeding), and vomiting.
- Acute Pain: She reports sharp, sudden, colicky abdominal pain localized in one side of the lower abdomen (iliac fossa).
- Referred Shoulder Pain: The mother complains of pain at the tip of her shoulder, especially when she lies down flat. This happens because the free blood pooling in her abdomen irritates the diaphragm muscle and the phrenic nerve, which shares a pain pathway with the shoulder.
On Physical Examination
- Signs of Pregnancy: Early signs may be visible, such as darkening of the breast areola.
- Signs of Shock: Because of massive internal bleeding, she will have cold and clammy skin, a rapid but very weak (thready) pulse, dangerously low blood pressure, and a slightly low temperature.
- Mental State: She appears highly anxious, restless, and terrified (air hunger).
- Pallor: Extreme whiteness (pallor) of the eyes, gums, and mucous membranes due to blood loss.
On Abdominal Palpation
- Extreme tenderness, especially on the affected side.
- The abdominal muscles become hard and rigid like a board because the mother is unconsciously guarding against the severe pain.
- The abdomen is visibly swollen (distended) due to the large amount of free blood floating in the abdominal cavity.
On Vaginal Examination
- Bleeding Discrepancy: The small amount of bleeding seen coming from the vagina absolutely does not match the mother's severe state of shock (because the real bleeding is hidden inside the abdomen).
- Cervical Excitation: Moving the cervix slightly during the exam causes her extreme, jumping pain.
- A distinct, painful swelling or mass can be felt on one side (lateral fornix) or bulging down behind the uterus in the Pouch of Douglas.
- Dark brown, old blood may be seen on the examining finger.
5. Investigations & Differential Diagnosis
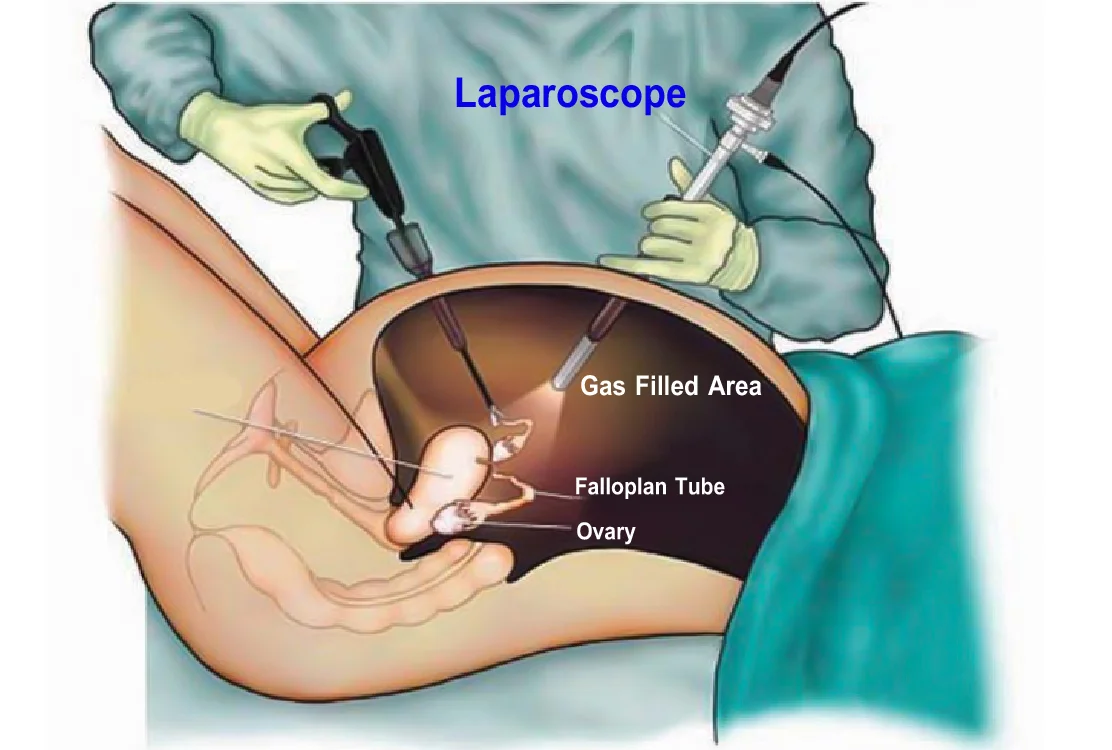
- Ultrasound Scan: This is the gold standard. It will confirm the diagnosis by revealing an empty uterus, a mass in the fallopian tube, and a large collection of free fluid/blood in the abdomen.
- Pregnancy Test: A urine or blood hCG test will be positive, proving she is pregnant.
- Blood Tests: Check Hb (Hemoglobin level will be very low due to bleeding), Grouping, and Cross-matching (to prepare for immediate blood transfusion).
- Culdocentesis (Emergency Puncture): If a scan is not available in a rural setting, a doctor may insert a needle through the top of the vagina into the Pouch of Douglas. If fresh, non-clotting blood is drawn out (aspirated), it proves there is internal bleeding from a rupture.
❓ Differential Diagnosis
Before confirming an ectopic pregnancy, a midwife or doctor must rule out other conditions that cause severe abdominal pain in women, including:
- Salpingitis / PID: Specially if associated with foul discharge and irregular menses.
- Appendicitis: Right-sided pain, often with a fever, but no missed period.
- Abortion (Miscarriage): Will have heavy vaginal bleeding matching the pain level.
- Twisted Ovarian Cyst: Sudden, severe pain, but pregnancy test is usually negative.
- Urinary Tract Infection (UTI): Pain on urination, usually no signs of severe shock.
6. Management at a Health Centre (Primary Care)
At a lower-level health center (Level III or IV), this is a critical emergency. Every second counts to save the mother's life. Do not delay.
Aims of Care: To prevent deep shock, relieve severe pain, reassure the terrified patient, and transfer her safely and immediately.
- Admission: Temporarily admit her to the gynecological or emergency bed. Quickly take a brief history and do a rapid physical, abdominal, and vaginal examination to make a diagnosis.
- Observations: Immediately take and record Temperature, Pulse, Respiration, and Blood Pressure to assess how badly her vital organs are failing.
- Resuscitation (Treatment):
- Put up an incredibly fast intravenous (IV) drip of Normal Saline to elevate her dropping blood pressure and treat the shock.
- Administer strong pain relief as prescribed (e.g., Morphine 15mg intramuscularly) to stop pain from worsening the shock.
- Raise the foot of the bed (Trendelenburg position) to force whatever blood is left to flow to her vital brain and heart centers.
- Nursing Care: Swab the vulva quickly and apply a clean pad to monitor exactly how much vaginal blood is lost during transit.
- Transport and Transfer: Inform the patient and her relatives honestly about the danger and the immediate need for surgery. Send for an ambulance or vehicle immediately. Write a detailed referral note stating the time of arrival, her exact condition, and what drugs/IV fluids you have given. A qualified midwife MUST escort the mother to monitor the IV drip and hand her over safely to the hospital staff.
7. Hospital Management
Upon arrival at a main hospital, this is handled as a top-priority gynecological emergency. All nurses and doctors must work as a rapid-response team to get the patient to the operating theatre as fast as possible.
Aims: To treat anemia, reverse shock, reassure the patient, completely stop the internal bleeding, and prevent further complications.
Admission and Immediate Care
- Admit the patient into a warm, well-ventilated room. Establish a fast but comforting nurse-patient relationship.
- Take a collateral history from the relatives if the mother is too weak to speak. Focus on exactly when the pain started, vomiting, and missed periods.
- Call the doctor or surgeon immediately.
- Do a rapid head-to-toe examination focusing on signs of extreme dehydration, anemia, and hypovolemic shock.
Doctor's Orders and Resuscitation
- Investigations Ordered: Hb estimation (to see blood lost and rule out malaria), Blood Group & Crossmatch (transfusion is almost always necessary), Pregnancy test, Ultrasound scan, and Urinalysis.
- IV Fluids & Fluid Balance: Run Normal Saline rapidly. Start a strict fluid balance chart (input vs. output).
- Blood Transfusion: Book 1 to 2 units of blood immediately based on the Hb results.
- Pain Relief: Administer strong analgesics like Morphine or Pethidine.
8. Pre-Operative, Theatre, and Post-Operative Care
Pre-Operative Care (Preparation for Theatre)
- Explain the life-saving nature of the operation and obtain a signed Informed Consent form from her or her husband.
- Give a quick bed bath, dress her in a clean theatre gown, and inform the theatre staff to prepare.
- Ensure the IV line is running perfectly. Swab the vulva to prevent taking infections into theatre.
- Pass a urethral catheter to empty the bladder (an empty bladder is out of the surgeon's way and prevents accidental injury).
- Pass a Naso-Gastric (NG) tube to empty stomach contents, or give an antacid (like Magnesium Trisilicate) to make stomach acid safe. This prevents the mother from vomiting and breathing acid into her lungs while unconscious.
- Give premedication like Atropine to dry up mouth and lung secretions.
- Take one last set of vital signs, gather all her medical charts, and carefully wheel her to theatre, giving a full verbal handover to the theatre nurse. Stay with her until she is asleep if possible.
🩸 What happens in Theatre? (Auto-transfusion)
The surgeon performs a Laparotomy (opening the abdomen) and a Salpingectomy (cutting out the burst fallopian tube). The bleeding is clamped and tied off. If the bleeding just happened and the blood in her stomach is totally fresh, the surgeon can scoop it up, filter (sieve) it, mix it with an anti-clotting chemical (Sodium Citrate), and give her own blood back to her through her IV line. This amazing life-saving trick is called Auto-transfusion.
Post-Operative Care (On the Ward)
While the mother is in surgery, the ward nurse prepares a special recovery bed equipped with an oxygen machine, drip stand, observation charts, and resuscitation tray.
- Receiving the Patient: Collect her from the recovery room. Check her Airway, Breathing, and Circulation (ABCs). Check her surgical wound for fresh bleeding. Check if the catheter is draining clear yellow urine.
- Positioning: Place her flat (recumbent) in the bed with her head turned to one side. This allows saliva to drain out and stops her tongue from falling back and choking her.
- Monitoring Vitals: Take her BP, Pulse, Respiration, and Temp every 15 minutes, then every 30 minutes, then every hour as she gets stronger. Continue this until she is discharged.
- Fluid/Hydration: Continue IV Normal Saline (0.9%). Monitor the cannula site for swelling. Stop IVs only when her intestines wake up (bowel sounds are heard) and she can drink safely.
Drug Therapy and Diet
The mother will be on a heavy regimen of drugs to ensure full recovery and prevent deadly infections inside her abdomen.
- Antibiotics: Ampicillin 500mg (6 hourly for 5 days), Ceftriaxone 2gm (once daily), Metronidazole 500mg (8 hourly), or Gentamycin 160mg (once daily).
- Painkillers: Pethidine 100mg (8 hourly for early severe pain), Diclofenac 75mg, then switch to oral Panadol 1gm (8 hourly) when she can swallow.
- Blood Builders: Ferrous sulphate and Folic acid to cure her severe anemia over the coming weeks.
- Diet: Once bowel sounds are positive, start with sips of water. Upgrade to soft foods rich in Proteins (for tissue repair), Roughage (to stop constipation), and Carbohydrates (for lost energy). Remove the NG tube.
- Physiotherapy: Force her to take deep breaths to prevent lung collapse (hypostatic pneumonia). Encourage her to wiggle her toes, then stand up and walk around quickly to prevent dangerous blood clots in her legs (Deep Vein Thrombosis).
- Wound & Hygiene Care: Check the dressing daily. Do not let it soak with blood. Stitches are usually removed on the 7th and 8th day. Give her a bed bath until she can walk to the shower. Remove the catheter in 24-48 hours. Give laxatives (Bisacodyl 5-10mg) if she cannot pass stool.
9. Advice on Discharge & Complications
Advice on Discharge
- Rest completely at home. Absolutely no heavy lifting or digging, to avoid bursting her healing abdominal muscles.
- Complete every single antibiotic pill given to her.
- Bring the husband in for STI treatment if Pelvic Inflammatory Disease (PID) caused the ectopic.
- She must attend the hospital immediately when she gets pregnant again, to verify the new baby is in the right place.
- Return to the clinic on her exact appointed review dates.
10. Medical Management of Ectopic Pregnancy (Methotrexate Therapy)
In modern midwifery, surgery is not always required for early, silent ectopic pregnancies. Methotrexate is a highly effective, non-surgical alternative that preserves the mother's fallopian tube, protecting her future fertility.
A. Patient Selection Criteria (Who Can Receive It?)
Not every ectopic pregnancy can be treated medically. The midwife must ensure the patient meets strict criteria before starting Methotrexate therapy:
- Hemodynamic Stability: The mother must have normal vital signs (stable blood pressure and heart rate) with absolutely no signs of internal bleeding, active rupture, or shock.
- Ectopic Mass Size: The adnexal mass containing the ectopic pregnancy must be small, typically less than 3.5 cm (35mm) on an ultrasound scan.
- Fetal Cardiac Activity: There must be no visible fetal heartbeat inside the ectopic sac on the ultrasound.
- Serum Beta-hCG Levels: Ideally, the baseline hCG level should be low. The absolute limit for medical management is < 5,000 mIU/mL (Success is highest when hCG is < 1,500 mIU/mL; success drops drastically if hCG exceeds 5,000 mIU/mL).
- Normal Organ Function: The mother must have healthy kidneys and liver. Liver Function Tests (LFTs) and kidney function (creatinine) must be normal. She must not have severe blood disorders (like deep anemia or thrombocytopenia).
- Patient Compliance: The mother must understand, agree to, and be physically able to return to the clinic for strict, repeated follow-up blood tests over several weeks.
⚠️ Absolute Contraindications to Methotrexate
Never administer Methotrexate to a mother who has: Ruptured ectopic pregnancy, active liver or kidney disease, severe anemia, active pulmonary (lung) disease, a compromised immune system, or who is currently breastfeeding (the drug passes into breast milk and is highly toxic to a baby).
B. Dosages and Administration Regimens
There are three standard clinical protocols used to administer Methotrexate:
- 1. Single-Dose Protocol (Most Common):
The patient receives a single intramuscular (IM) injection of Methotrexate at a dose of 50 mg/m² (calculated using the mother's body surface area based on her height and weight). It is injected into the gluteal muscle (buttock) or thigh.
- 2. Two-Dose Protocol:
Given as a 50 mg/m² IM injection on Day 1, followed by a second 50 mg/m² IM injection on Day 4. This is often used if the starting hCG levels are moderately high.
- 3. Multi-Dose Protocol (Fixed Regimen):
Alternating injections of Methotrexate (1 mg/kg IM) on Days 1, 3, 5, and 7, alternated with Leucovorin (Folinic Acid) 0.1 mg/kg IM on Days 2, 4, 6, and 8. Leucovorin acts as a "rescue drug" to protect the mother's healthy liver and bone marrow from the harsh effects of Methotrexate.
C. Follow-up Protocol: The 15% Rule
The midwife must follow a highly strict monitoring timeline to confirm that the medicine is working successfully:
| Day of Protocol | Clinical Action & Expected Findings |
|---|---|
| Day 1 | Draw blood for a baseline serum beta-hCG test. Give the first IM injection of Methotrexate. (Give Rhogam injection if the mother has an Rh-negative blood type). |
| Day 4 | Draw blood for a second beta-hCG test.
Note: It is normal for the hCG level to rise or stay flat on Day 4. This happens because the dying pregnancy cells are breaking open (lysing) and dumping their hormones into the bloodstream. Do not panic if the level is higher than Day 1. |
| Day 7 | Draw blood for a third beta-hCG test. |
| Day 7 Evaluation | Compare the hCG levels of Day 4 and Day 7.
There must be a decrease of at least 15% between the Day 4 and Day 7 readings. |
| Weekly Follow-up | If the 15% drop is successful, the patient must return every 7 days for a repeat hCG blood draw. This must continue weekly until the hCG level drops to a non-pregnant level (typically < 5 mIU/mL). This process can take anywhere from 2 to 6 weeks. |
🚫 Crucial Patient Care Instructions
While undergoing Methotrexate therapy, the mother must be strongly counseled to:
- DO NOT take folic acid or prenatal vitamins: Folate blocks the action of the drug and will make the treatment fail.
- Avoid gas-producing foods: Stomach gas causes sharp abdominal pain, which can be easily confused with a ruptured fallopian tube.
- Avoid aspirin and NSAIDs (like Ibuprofen): These can react poorly with Methotrexate and cause liver or kidney strain. Use Paracetamol for mild pain.
- Avoid sunlight: Methotrexate makes the skin highly sensitive to sun, leading to fast, painful sunburns.
- Avoid vigorous exercise and sexual intercourse: Hard physical pelvic movement can physically trigger the fragile tube to rupture.
- Use strict birth control for 3 to 6 months: If she gets pregnant immediately after taking Methotrexate, the drug can cause severe, fatal birth defects in the new baby.
D. When Has Medical Management Failed? (Indications for Surgery)
The midwife must immediately take the patient to the operating theatre for emergency surgery (Laparotomy and Salpingectomy) if any of the following signs of treatment failure occur:
- Worsening Abdominal Pain: Sharp, severe, or worsening lower abdominal pain with rigid, guarded abdominal muscles. This is a primary warning sign that the tube has ruptured and she is bleeding internally.
- Hemodynamic Instability: Sudden signs of shock, such as a drop in Blood Pressure (hypotension), a rapid thready pulse (tachycardia), and cold, clammy skin.
- Suboptimal hCG Drop: If the beta-hCG level fails to drop by at least 15% between Day 4 and Day 7:
- If she is still asymptomatic and completely stable, a second dose of Methotrexate may be administered.
- If the hCG levels still fail to drop after the second dose, or if she develops pain, she must go straight to surgery.
Complications of Ectopic Pregnancy
| Immediate Complications | Long-Term Complications |
|---|---|
| Hypovolemic Shock (from massive blood loss) | Chronic Pelvic Sepsis / Infection |
| Peritonitis (inflammation of the abdominal cavity from old blood) | Severe Chronic Anaemia |
| Severe Dehydration | Fibrosis and massive abdominal adhesions |
| Death (if not operated on rapidly) | Recurrence (high risk of another ectopic pregnancy) |
| Secondary Infertility (struggling to get pregnant again because one tube is gone and the other may be damaged) |

Thanks it’s very helpful
This is beautiful ❤️