
Examination of the Placenta
The word Placenta is derived from the Greek word "plakuos," meaning "flat cake," which perfectly describes its typical shape. It is a vital fetal organ responsible for providing nutrition, oxygen, and excretory functions to the growing fetus.
Embryology: It is formed by both maternal and fetal components:
- Maternal Component: Decidua placentalis (formed by trophoblastic invasion of the endometrium).
- Fetal Component: Chorion frondosum (formed by branches of the umbilical artery protruding into intervillous spaces).
A quick, one-minute clinical examination in the delivery room provides crucial information for the immediate care of both the mother and the newborn.
1. Aims of Placenta Examination
Every midwife must carefully examine the placenta immediately after it is delivered to achieve two primary goals:
- To determine completeness: Ensuring that no part of the placenta, cotyledons, or membranes is left inside the mother's uterus, which could cause fatal postpartum hemorrhage (PPH) or sepsis.
- To detect abnormalities: Identifying any structural defects, tumors, nodules, or signs of infection that are associated with abnormal fetal development and perinatal morbidity.
Gross Anatomy of a Normal Term Placenta
Before looking for abnormalities, a midwife must know what a normal, healthy placenta looks like:
- Size and Weight: A fresh, term placenta measures approximately 15 to 22 cm in diameter and weighs between 470g and 600g (roughly 1/6 of the baby's total birth weight).
- Thickness: It is normally 2.0 to 2.5 cm thick. Interestingly, placental thickness is directly proportional to the gestation age (e.g., a 21-week placenta will be about 21 mm thick).
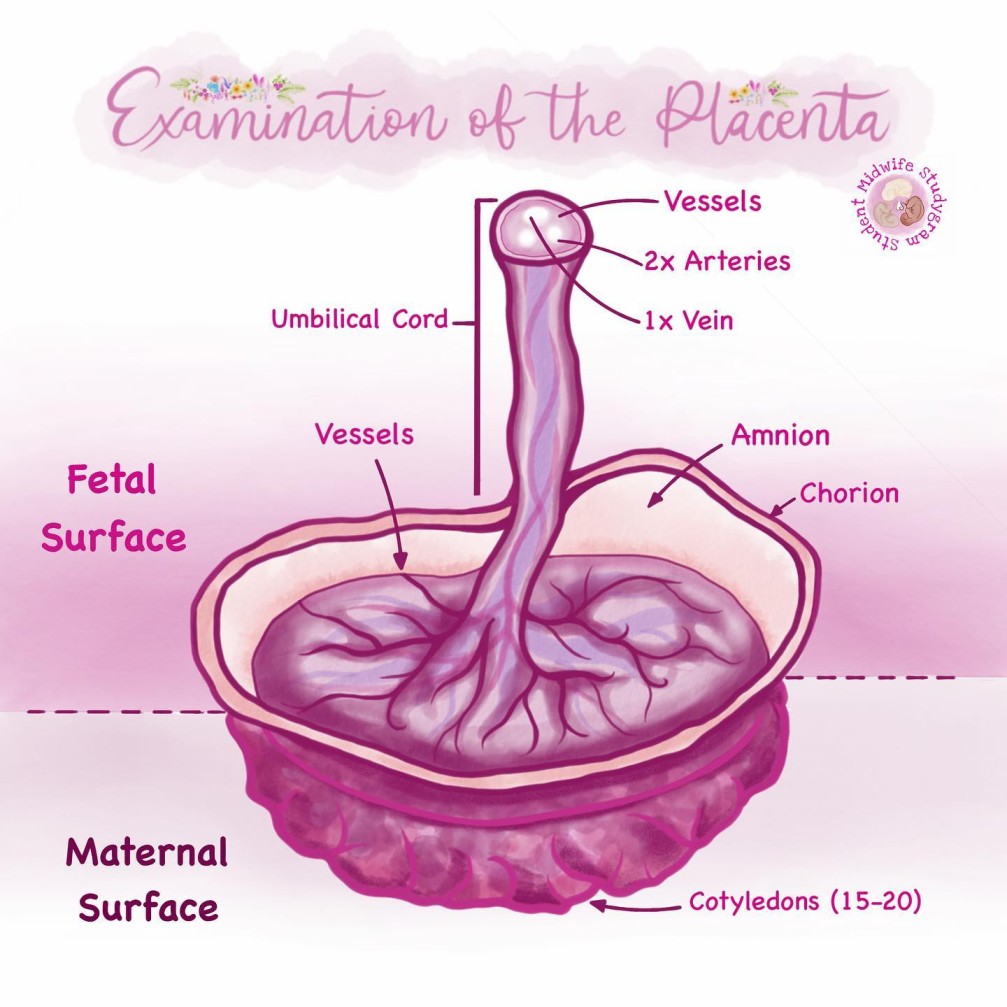
- Maternal Surface: Should be a dark maroon color, consisting of around 20 lobes (cotyledons) that fit perfectly together with no missing gaps.
- Fetal Surface: Should be shiny, gray, and translucent (clear) enough that the underlying maroon tissue can be seen.
2. Requirements and Preparation
To safely examine the placenta without causing blood spillage or infection, the midwife must organize the following equipment:
| Location | Equipment Required |
|---|---|
| Top Shelf |
|
| Bottom Shelf |
|
| At the Side |
|
3. Procedure for Examination
The examination should be done systematically. Always begin by explaining the procedure to the mother and guardian, and ask if they wish to observe.
Step 1: Inspecting the Fetal Surface and Membranes
- Initial Lay Out: Wear your protective gear. Lay the placenta flat on the surface with the fetal side uppermost. Note the overall size, shape, smell, and color.
- Check for Irregularities: Look for fatty deposits, infarctions (dead tissue), or the presence of large (velamentous) blood vessels running unprotected through the membranes.
- Lift and Inspect Holes: Hold the placenta up by the umbilical cord. This allows the membranes to drop down like a bag. There is normally only a single hole where the baby passed through. If you see extra holes or torn vessels leading nowhere, suspect a missing Succenturiate lobe (an extra accessory lobe left in the uterus).
- Separate the Layers: Return the placenta to the flat surface. Gently pull the inner membrane (amnion) back over the base of the umbilical cord to separate it from the outer membrane (chorion). Ensure both layers are fully present.
Step 2: Examining the Umbilical Cord
- Length and Insertion: Note the total length of the cord and exactly where it inserts into the placenta (central, marginal/battledore, or velamentous).
- Count the Vessels: Inspect the freshly cut end of the cord. The normal cord contains two arteries and one vein. Clinical Tip: Count the vessels in the middle or fetal third of the cord, because arteries sometimes fuse near the placenta, making them difficult to differentiate.
- Look for Abnormalities: Check the cord for true knots, thromboses (blood clots blocking the cord), and the healthy presence of Wharton's jelly (the protective jelly around the vessels).
🧠 Memory Aid for Umbilical Cord Vessels
Remember the word AVA to recall the normal blood vessels in the umbilical cord:
A = Artery
V = Vein (The single, largest one)
A = Artery
Step 3: Inspecting the Maternal Surface
- Turn it Over: Carefully turn the placenta over to inspect the dark maroon maternal surface.
- Piece it Together: Gently push the lobes (cotyledons) together. A complete placenta will fit neatly together without any gaps, with the edges forming a uniform circle. Broken fragments must be carefully replaced to make an accurate assessment.
- Check for Missing Tissue: Ensure all roughly 20 cotyledons are present. Tissue may be retained inside the mother due to abnormal lobation or conditions like placenta accreta (where the placenta grows too deeply into the uterine wall).
- Remove Clots: Remove any blood clots from the maternal surface and place them in the measuring jar to accurately assess the mother's total blood loss.
4. Clinical Interpretations of Abnormal Findings
A trained midwife uses the placenta to read the story of the pregnancy. Any of the following abnormal findings must be documented, and the placenta should be submitted for pathologic evaluation.
Placental Size and Thickness
- Less than 2.0 cm thick: Strongly associated with Intrauterine Growth Retardation (IUGR) of the fetus.
- More than 4.0 cm thick: Associated with maternal diabetes mellitus, fetal hydrops (fluid buildup in the baby), and severe intrauterine fetal infections.
Surface Abnormalities
- Pallor (extreme paleness) of the maternal surface: Indicates fetal anemia, which may be a sign of active fetal hemorrhage (such as in vasa previa). With prompt recognition, a lifesaving blood transfusion can be arranged for the newborn.
- Clots on the maternal surface: Adherent, centrally located clots usually represent Placental Abruption (premature separation of the placenta).
- Thick ring of membranes on the fetal surface: Represents a Circumvallate Placenta. This is dangerously associated with prematurity, prenatal bleeding, multiparity, and early fluid loss.
- Thin ring of membrane tissue: Represents a milder condition called a Circummarginate Placenta.
Umbilical Cord Abnormalities
A normal umbilical cord measures between 40 cm and 70 cm.
- Short Cord (Less than 40 cm): Associated with a less active fetus, fetal malformations, Down syndrome, neuropathic diseases, and oligohydramnios (low amniotic fluid).
Risks during labour: Cord rupture, bleeding, prolonged second stage of labour, uterine inversion, and placental abruption. - Long Cord (More than 70 cm): Associated with fetal hyperkinesis (excessive movement).
Risks: Severe entanglements around the baby's neck, torsion (twisting), true knots, and thromboses. - Missing a Vessel (Single Umbilical Artery): If only one artery and one vein are grossly visible, the fetal anomaly rate is nearly 50 percent. These anomalies heavily affect the newborn's cardiovascular, genitourinary, and gastrointestinal systems.
Fetal Membrane Odors
Normal membranes are thin, gray, and glistening. Thick, dull, discolored, or foul-smelling membranes indicate strong possibilities of infection. The specific smell gives the midwife a clue to the bacteria:
- Fecal odor (smells like stool): May indicate infection by Fusobacterium or Bacteroides.
- Sweet odor: May indicate infection by dangerous bacteria like Clostridium or Listeria.
⚠️ Attention: Incomplete Placenta
Where there is any suspicion that the placenta and/or the membranes are incomplete, they must be kept for further inspection and the duty obstetrician/doctor must be informed immediately. Inform the mother of the findings and complete the documentation in her health care record.
5. Disposal of the Placenta
- Cultural Considerations: Always politely inquire from the mother if she would like to take the placenta home, as many cultures have specific burial traditions for it.
- Medical Disposal: If the mother declines, dispose of the placenta by taking it directly to the hospital's incinerator or the designated biological placenta pit. Wash hands thoroughly and sanitize the work area.
💡 Quick Practice Check
Question: While examining the cut end of an umbilical cord, the midwife notices there is only one large vein and one artery present. What is the immediate clinical concern?
Answer: A Single Umbilical Artery carries a 50% risk of fetal anomalies, specifically affecting the baby's cardiovascular, gastrointestinal, and genitourinary systems. A thorough pediatric assessment of the newborn is required.

Good lessons taught
Need more of this examination
Quite comprehensive ❤️!