
Normal Puerperium
1. Phases, Principles, and Aims of Puerperium
The Three Phases of Puerperium
- Immediate Puerperium: The initial phase spanning the first 6 hours after childbirth.
- Early Puerperium: The second phase extending up to 6 days postpartum.
- Remote Puerperium: The final healing phase continuing up to 6 weeks after childbirth.
Principles of Management
The care provided to a mother during the puerperium is guided by several essential principles:
- Restoring the mother’s health and energy to optimal levels.
- Preventing infections by ensuring a strictly hygienic environment.
- Providing proper care for the breasts to facilitate smooth and successful breastfeeding.
- Encouraging the mother to consider contraceptive options to space out future pregnancies (Family Planning).
Aims of Management
The midwife focuses on achieving the following goals:
- Establishing the complete physical and emotional well-being of the mother.
- Facilitating lactation to promote exclusive breastfeeding.
- Educating the mother on the best, safest practices for caring for her newborn baby.
- Preventing any life-threatening complications that may arise during this period (e.g., bleeding or sepsis).
2. Management in the 1st Hour (Fourth Stage of Labor)
The fourth stage of labor begins immediately with the birth of the placenta and lasts for exactly one hour. This is a highly critical phase where the mother recovers from the extreme physical stress of labor and delivery. Close monitoring must be conducted.
Evaluation of the Uterus
- Palpating the uterus: Feel the abdomen to ensure the uterus is hard and properly contracted (like a firm grapefruit).
- Massaging the fundus: Gently rub the top of the uterus to expel any trapped blood clots and promote the shrinking process (uterine involution).
- Measuring fundal height: Check the height of the uterus in relation to the mother's umbilicus (belly button).
- Emptying the bladder: Encourage the mother to urinate. A full bladder blocks the uterus from contracting tightly and causes heavy bleeding.
Inspection of the Perineum, Vagina, and Cervix
- Carefully inspect the perineum for unusual discoloration, heavy swelling (hematoma), lacerations, or deep tears.
- When to examine the cervix and upper vagina: A deep examination is required if you notice any of the following factors:
- The uterus is well-contracted and hard, but there is still continuous bright red vaginal bleeding for an hour. (This usually means the cervix or vagina is torn).
- The mother started pushing before the cervix was fully dilated (10cm).
- The labor was unusually rapid and precipitous (very fast delivery).
- There was manual manipulation of the cervix during labor, such as the midwife pushing back a swollen (edematous) anterior lip.
- Traumatic procedures were used, like a forceps delivery.
- The delivery was very traumatic, such as delivering a very large baby or dealing with stuck shoulders (shoulder dystocia).
Inspection of the Placenta and Post-Delivery Care
- Placenta, Membranes, and Cord: Examine the placenta carefully to ensure no pieces are left inside the womb. This must be done before any repairs (like stitching a tear or episiotomy) are started.
- Cleaning: Wash the perineum gently with warm water, dry it, and position the mother's legs comfortably.
- Observations: Continuously monitor and record vital signs: Blood Pressure (BP), Pulse, Temperature, and Respiration (TPR).
- Food and Fluids: Provide warm, sweet drinks and nourishing food to restore the mother's energy. Ensure she is covered and stays warm.
- Breastfeeding: Help the mother put the baby to the breast immediately. This promotes deep emotional bonding and triggers hormones (oxytocin) that start milk flow and contract the uterus.
At the end of this first hour, repeat all observations. If the mother is stable, she and her baby are transferred to the postnatal ward for ongoing care.
3. Management in the Postnatal Ward (First 6 Hours)
Upon arriving at the postnatal ward, the mother is very tired and highly susceptible to bleeding. The ward must be ready to welcome her and make her comfortable.
- Rest and Sleep: Deep rest is crucial for recovery. Visitors must be strictly limited during the day to reduce anxiety, noise, and discomfort. Maintain a calm atmosphere. If the mother cannot sleep at all, a doctor may prescribe mild sedatives to prevent exhaustion and address early signs of puerperal psychosis (severe mental confusion).
- Ambulation (Walking): After 6 hours of a normal delivery, the mother must be encouraged to get out of bed and walk around the ward. Walking promotes good blood circulation, helps the heavy vaginal blood (lochia) drain out, and speeds up the shrinking of the uterus (involution). It also improves muscle tone and pumps blood back up from the legs, drastically reducing the risk of deadly blood clots (Deep Vein Thrombosis - DVT).
- Diet and Fluids: Provide a well-balanced diet rich in proteins, vitamins, and nutrients to help her regain strength and produce rich breast milk. Encourage her to drink plenty of fluids to prevent hard stool (constipation). Continue giving Vitamin, Iron, and Folic Acid supplements as needed.
- Care of the Bladder: The mother excretes very large amounts of urine in the early days of puerperium as the body drops water weight. She might struggle to pass urine because of bruising, pain, or lack of privacy. Ensure she empties her bladder regularly. A full bladder causes a dangerous chain reaction: it stops the uterus from shrinking (subinvolution), which leads to severe Postpartum Hemorrhage (PPH) and Urinary Tract Infections (UTIs).
- Hygiene: "Vulval toilet" (cleaning the genital area) should be performed at least 3 times a day. Pads must be changed immediately whenever soiled. Encourage daily warm baths and fresh, clean clothing and bed sheets. Provide a clean, suitable bathroom.
- General Examination: The midwife must do a daily head-to-toe check. Look for pale eyes (anemia), swollen legs/face (edema), yellow eyes (jaundice), and dry lips (dehydration). Use a tape measure to check fundal height daily. Inspect the vulva and check the vaginal discharge (lochia) for its color, amount, and smell (a foul smell means infection). Squeeze the calf muscles to check for pain, a sign of Deep Vein Thrombosis (DVT).
- Care of Breasts: Breasts should be wiped clean with water before feeding. Immediate and frequent breastfeeding prevents severe bleeding (PPH). The midwife must supervise and assist the mother to ensure the baby attaches (latches) properly. "Demand feeding" (feeding whenever the baby cries) keeps the milk flowing and prevents painful, swollen breasts (engorgement). Advise the mother to wear a well-fitting brassiere for support.
- Relief of Pain: Mothers (especially those who have had previous babies) will experience sharp, cramp-like "after-pains" as the uterus aggressively contracts for the first 2-3 days. Provide pain relief like Paracetamol (Panadol).
- Perineal Care: Inspect the perineal pad constantly. The mother must avoid sexual intercourse (coitus) for up to 6 weeks, or until the perineum has fully healed. Strongly discourage the application of traditional/native medicines on the wound, as they cause severe infections. Teach postnatal exercises.
4. Vulval Toilet & Postnatal Care Procedure
To prevent infection, cleaning the mother's genital area is treated as a sterile clinical procedure.
Requirements: The Trolley Setup
| Top Shelf (Sterile Items) | Bottom Shelf (Clean Items) | Bedside Equipment |
|---|---|---|
|
Sterile dressing pack containing: - 2 dressing towels - 2 non-toothed dissecting forceps - 2 dressing forceps - 3 gallipots (1 for lotion, 1 for swabs, 1 for gauze) - A pair of stitch scissors / clip remover (if needed) - Probe - Sinus forceps |
- Sterile drum of cotton wool - Sterile drum of gauze - 2 flannels - Antiseptic solution & Normal saline - Bathing soap - Dressing mackintosh and towel - Plastic Apron - Clean Gloves - Cheatle forceps - 2 clean sanitary towels - 2 jugs of water (1 hot, 1 cold) - A small jar for pouring water - 2 empty receivers (kidney dishes) |
- Privacy Screen - Bedpan and bedpan cover - Hand washing equipment (water and soap) - Linen hamper for dirty clothes/sheets |
Step-by-Step Procedure
- Request the mother to empty her bladder and bowel before starting.
- Fold back the bedclothes to the foot of the bed, leaving the patient covered only up to the waist with a top sheet to preserve dignity.
- Put the mother in a dorsal position (lying flat on her back with knees bent and parted).
- Wash your hands, put on clean gloves, and carefully remove her soiled sanitary pad, noting its contents before disposing of it properly.
- Inspect the genitalia directly for any signs of swelling, broken stitches, or infection.
- Examine the lochia (vaginal discharge), noting its exact amount, color, consistency, and odor.
- Slide a bedpan securely under the mother's buttocks.
- Wash the pubic area (front), the inner parts of the thighs, and the buttocks using warm soapy water and a flannel.
- Carefully wash the actual genitalia. Use your dominant hand to gently cleanse with swabs while your non-dominant hand pours the warm water. Pay special attention to skin folds, and always clean from front to back.
- Rinse the area with clean water and dry it thoroughly, always moving from the perineum towards the rectum using a clean flannel or sterile swabs.
- Carefully remove the bedpan.
- Place a fresh, clean sanitary pad in position and ensure the mother’s clothes are pulled down and she is entirely comfortable.
- Clear away the trolley, clean the equipment, and wash your hands.
- Document the entire procedure, noting the state of the perineum and the lochia in the patient's medical records.
🧼 Patient Education: Self-Cleansing Instructions
Before leaving, clearly instruct the woman on how to cleanse herself after using the toilet:
- Always wash hands thoroughly before and after touching the perineal area.
- Never touch the stitches with bare fingers.
- Always use a wet wipe or water to clean from the front (vagina) to the back (anus). Never wipe back to front, as this drags feces into the healing birth canal.
- Apply the sanitary pad firmly so it doesn't slide around when moving.
- When removing a soiled pad, pull it downwards and backward (front to back).
5. Ongoing Postnatal Care
- Postnatal Exercises: These are critical for proper blood circulation and for bringing strength (tone) back to stretched abdominal and pelvic floor muscles. Exercises include deep breathing, free leg movements in bed, relaxation techniques, and squeezing the pelvic floor (Kegel exercises).
- Observations: The mother's Temperature, Pulse, Respiration (TPR), and Blood Pressure (BP) must be checked and recorded twice a day.
- Care of the Bowel: Digestion and bowel movements become very slow (sluggish) in the first 2 days. Constipation must be aggressively avoided because a bowel full of hard stool presses on the uterus, contributing to subinvolution. Provide high-roughage foods and plenty of water. If needed, give a mild laxative like Milk of Magnesia.
- Prevention of Infection: Strict aseptic (sterile) precautions must be observed. Ensure proper use of gowns, masks, and gloves, and sterilize equipment. No healthcare worker or visitor with a cold, cough, or septic skin spot should be allowed near a puerperal mother. Keep visitor numbers low.
- Rooming-In / Bedding-In: The baby should never be kept in a separate nursery. The baby must stay in a cot directly beside the mother’s bed or in her bed when she is awake. This triggers maternal instincts, promotes deep bonding, and helps her learn baby care quickly.
- Immunization for the Mother: If the mother is susceptible to Rubella, she should be vaccinated, but must be strictly advised to postpone getting pregnant again for at least 2 years. Give a Tetanus Toxoid (TT) shot at discharge if she missed it during pregnancy. Crucial: If the mother's blood type is Rh-Negative and she just delivered an Rh-Positive baby, she MUST receive an Anti-D injection within 72 hours to protect her future pregnancies.
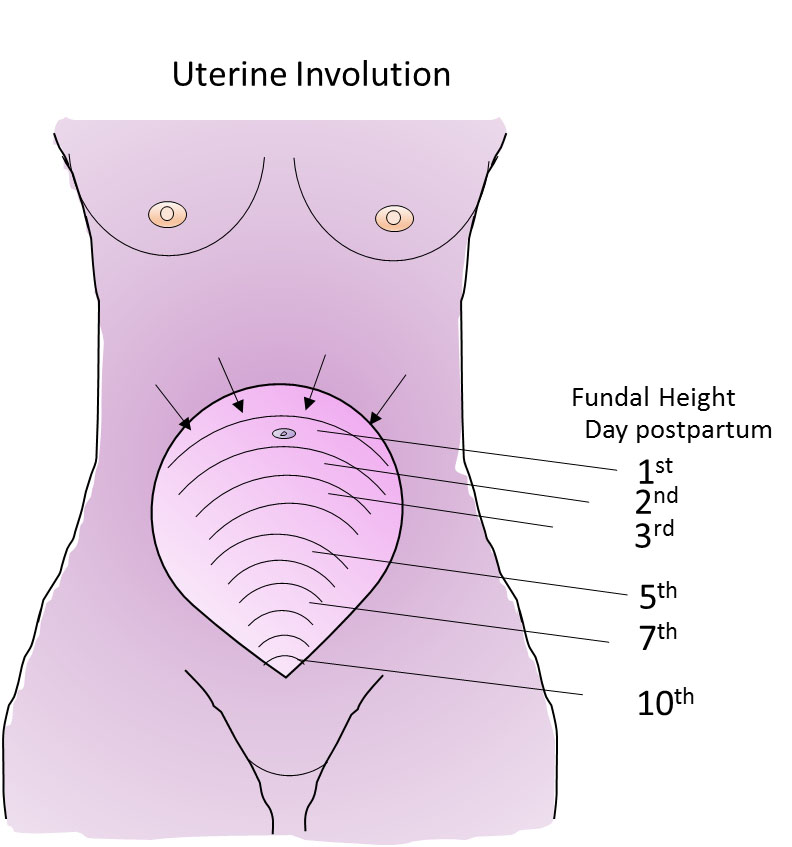
Involution of the Uterus
Involution is the rapid shrinking of the uterus. Daily palpation of the fundus is essential. The uterus should feel smooth, very firm, well-contracted, and should not be extremely painful to touch. The midwife must measure the fundal height daily using a tape measure (it should drop by about 1 finger-width or 1cm per day).
🚨 Warning Sign: Subinvolution
If the uterus remains the exact same size for several days, feels soft and boggy, or is painful, it is failing to shrink. This is called Subinvolution, often caused by a full bladder, retained placental pieces, or infection. It is a major cause of late postpartum hemorrhage.
6. Discharge of the Mother and Baby
Before anyone goes home, both the mother and the baby must be fully examined to confirm they are 100% healthy and stable.
- For the Mother, the midwife checks: All vital signs are normal, breasts are soft (not engorged) and milk is flowing, the uterus is involuting properly, the lochia is normal (no bad smell or heavy bleeding), the bladder and bowels are functioning smoothly, and the perineal wound is clean and intact.
- For the Baby, the midwife checks: The baby is sucking well at the breast, has a normal sleeping pattern, the umbilical cord stump is clean and dry, and all birth vaccines (BCG for Tuberculosis and Polio 0) have been given.
Comprehensive Advice on Discharge
Advice for the Mother
- Personal Hygiene & Breast Care: Continue bathing daily. Keep the perineal area dry. Cleanse the breasts with clean water before and after every single feed.
- Diet: Eat a highly nutritious, well-balanced diet rich in proteins, vegetables, and fluids to support rapid tissue recovery and strong milk production.
- Rest and Sleep: Sleep whenever the baby sleeps. Exhaustion ruins milk supply and slows down healing.
- Postnatal Exercises: Continue doing Kegel exercises and mild walking to tone muscles and boost blood flow.
- Avoid Heavy Lifting: Do not lift anything heavier than your baby for the first 2-3 weeks to avoid straining the healing pelvic floor and abdominal muscles.
- Medications: Finish all prescribed medications (like antibiotics or iron tablets) exactly as directed.
- Vaginal Discharge & Menstruation: Understand that the lochia will change color (red to brown to white) and gradually stop. Her normal menstrual periods may return within 2-3 months, but might be delayed for several months if she is exclusively breastfeeding.
- Sexual Intercourse: Strictly avoid sex for about 6 weeks to allow bruised, torn, or stitched tissues to heal safely and perfectly.
- Postnatal Clinic: Emphasize that she absolutely must return to the clinic for a final check-up at exactly 6 weeks after delivery.
Advice for the Baby
- Exclusive Breastfeeding: Feed the baby ONLY breast milk for the first 6 full months. No water, no porridge. This provides optimal nutrition and heavy immune protection.
- Bottle Feeding (If medically necessary): Teach the mother exactly how to prepare formula safely. Explain how to boil and sterilize bottles, nipples, and spoons. Demonstrate holding the bottle tilted so the nipple is always full of milk, preventing the baby from swallowing painful air.
- Burping: Always hold the baby upright against the shoulder and gently pat the back after every feed to release swallowed gas.
- Bathing and Dressing: Show her how to gently sponge bathe the baby, keeping the baby warm. Teach her to carefully clean the baby's genital area (wiping front to back for girls).
- Cord Care: Keep the umbilical cord stump exposed to air, clean, and completely dry to prevent deadly tetanus or sepsis. Do not apply dung, herbs, or ash.
- Diaper Rash: Teach her to change wet/soiled diapers immediately, wash the buttocks with water, dry thoroughly, and apply a barrier cream (like Vaseline) to treat or prevent rashes.
- Baby's Temperature: Teach her how to feel the baby's chest or back to check for fever, and keep the baby warmly wrapped but not overheating.
- Recognizing Cues: Help the mother understand the different ways her baby cries to signal hunger, need for sleep, a wet diaper, or pain.
- Immunization Schedule: Stress the massive importance of returning to the clinic at 6 weeks, 10 weeks, and 14 weeks for the baby's routine vaccinations to protect against childhood diseases.
