Anthrax is a serious infectious disease caused by the bacterium Bacillus anthracis.
It’s a zoonotic disease, meaning it can be transmitted from animals to humans. While rare in humans, anthrax remains a significant public health concern due to its potential for use as a bioweapon.
Etiology
Bacillus anthracisis a Gram-positive, rod-shaped bacterium that forms highly resistant spores.
These spores can survive in soil and on animal products for extended periods, even decades. When conditions become favorable (e.g., entry into a living host), the spores germinate into vegetative bacteria, which then produce toxins responsible for the disease’s pathogenesis. The toxins include edema toxin, lethal toxin, and protective antigen. These toxins disrupt cellular processes, leading to the characteristic symptoms of anthrax.
Forms of Transmission and Routes of Transmission:
Anthrax primarily occurs in three forms, each with its characteristic route of transmission: These are also the types of Anthrax
Cutaneous Anthrax: This is the most common form in humans. It occurs when spores enter the body through a break in the skin, often through contact with infected animals or contaminated animal products (e.g., hides, wool, hair). The spores germinate in the skin, leading to the development of a characteristic lesion.
Inhalation Anthrax: This is the most dangerous form. It occurs when spores are inhaled into the lungs. Inhalation anthrax typically starts with flu-like symptoms, but rapidly progresses to severe respiratory distress and potentially fatal sepsis. This route is less common than cutaneous anthrax but carries the highest mortality rate.
Gastrointestinal Anthrax: This is the rarest form. It occurs when spores are ingested, usually through consumption of contaminated meat. Symptoms include nausea, vomiting, abdominal pain, and bloody diarrhea. This form also has a high mortality rate if untreated.
Incubation Period:
The incubation period varies depending on the form of anthrax and the route of infection:
Cutaneous Anthrax: 1-7 days (typically 2-5 days)
Inhalation Anthrax: 1-60 days (typically 1-7 days)
Gastrointestinal Anthrax: 1-7 days (typically 1-5 days)
Clinical Features
The clinical presentation varies widely depending on the type of anthrax:
Cutaneous Anthrax: Begins as a painless papule (pimple-like lesion) that develops into a vesicle (blister) and then an ulcer with a characteristic black eschar (scab). Other features may include lymphadenopathy (swollen lymph nodes), edema, and fever.
Inhalation Anthrax: Initial symptoms are flu-like (fever, cough, fatigue, muscle aches). This progresses to more severe symptoms, including shortness of breath, chest pain, respiratory distress, shock, and disseminated intravascular coagulation (DIC).
Gastrointestinal Anthrax: Severe abdominal pain, nausea, vomiting, bloody diarrhea, and potentially fatal sepsis.
Definitive Diagnosis and Investigations:
Diagnosis relies on a combination of clinical presentation, epidemiological information, and laboratory tests:
Clinical Examination: Careful assessment of the patient’s symptoms and medical history is crucial.
Microscopic Examination: Gram staining of clinical specimens (blood, wound fluid, etc.) may reveal the characteristic Gram-positive bacilli.
Culture: Isolation and identification of B. anthracis from specimens is definitive. High biosafety level is required.
Serological Tests: Detection of antibodies against B. anthracis toxins can be helpful but is not always definitive.
PCR: Polymerase chain reaction can detect B. anthracis DNA in clinical samples.
Management:
Aims of Management:
To eliminate the infection.
To neutralize the toxins produced by B. anthracis.
To provide supportive care to manage complications.
Medical Management:
The cornerstone of anthrax treatment is antibiotic therapy:
First-line: Ciprofloxacin (or other fluoroquinolones) or doxycycline.
Alternative: If the patient is allergic to fluoroquinolones, other antibiotics such as penicillin, clindamycin, or vancomycin may be used.
Duration: Antibiotics are typically administered for 60 days.
Cutaneous
95% of anthrax infections occur through skin cut or abrasion
Starts as raised itchy bump that resemble an insect bite
Within 1-2 days, it develops into a vesicle and then a painless ulcer, usually 1-3 cm in diameter, with a characteristic black necrotic (dying) area in the centre (eschar)
Lymph glands in adjacent area may swell
About 20% of untreated cutaneous anthrax results in death
First line is ciprofloxacin 500 mg every 12 hours
Alternatives: doxycycline 100 mg every 12 hours Or amoxicillin 1 g every 8 hours
Inhalation
Initial symptoms resemble a cold
After several days, symptoms may progress to severe breathing problems and shock.
Inhalation anthrax is usually fatal.
In addition to antibiotics, patients with inhalation anthrax may require supportive care including oxygen therapy, mechanical ventilation, fluid resuscitation, and treatment for shock and DIC. Raxibacumab (a monoclonal antibody targeting protective antigen) may be given in severe cases of inhalation anthrax.
Gastrointestinal
Acute inflammation of the intestinal tract
Initial signs of nausea, loss of appetite, vomiting and fever
Then abdominal pain, vomiting blood, and severe diarrhoea
Intestinal anthrax results in death in 25% to 60% of the cases
Nursing Care:
Nursing care focuses on:
Monitoring vital signs: Closely monitor the patient’s respiratory status, blood pressure, heart rate, and temperature.
Respiratory support: Provide oxygen therapy and assist with mechanical ventilation if necessary.
Fluid and electrolyte balance: Maintain adequate hydration and monitor electrolyte levels.
Wound care: For cutaneous anthrax, provide appropriate wound care to promote healing.
Infection control: Strict adherence to infection control protocols to prevent transmission.
Psychological support: Provide emotional support to the patient and their family.
Management up to Discharge:
Continue antibiotic therapy as prescribed. Monitor for any signs of relapse or complications. Provide patient education on medication, wound care (if applicable), and follow-up appointments.
Advice on Discharge:
Complete the entire course of antibiotics.
Monitor for any recurrence of symptoms.
Report any new symptoms to healthcare provider.
Follow-up appointments as scheduled.
Prevention:
Animal-focused Prevention:
Safe Carcass Disposal: Proper burial of animal carcasses, hides, and skins is crucial. Burning is ineffective as it can aerosolize spores, increasing the risk of spread.
Avoidance of Handling: Do not skin or handle dead animals suspected of anthrax infection, as this allows spore formation, which can persist in the soil for decades. Meat from such animals should never be consumed.
Movement Restriction: Restrict the movement of animals and animal by-products (e.g., hides, wool) from infected to unaffected areas to prevent disease spread.
Mass Animal Vaccination: Implement widespread vaccination programs for livestock in areas with a history of anthrax outbreaks.
Human-focused Prevention:
Vaccination: Human anthrax vaccination is recommended for individuals at high risk of exposure, including:
Laboratory personnel working directly with Bacillus anthracis.
People residing in or visiting high-incidence areas.
Health Education: Public health campaigns should educate communities about anthrax transmission, prevention, and early recognition of symptoms. This includes safe handling practices for animal products and seeking immediate medical attention if exposure is suspected.
Complications:
Sepsis: A life-threatening complication that can occur in any form of anthrax.
Respiratory failure: A common complication in inhalation anthrax.
Meningitis: Inflammation of the meninges (protective membranes surrounding the brain and spinal cord).
Shock: A life-threatening drop in blood pressure.
DIC: Disseminated Intravascular Coagulation.
Death: The mortality rate is high for untreated inhalation and gastrointestinal anthrax.
Quick Quiz
Anthrax Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Tetanus is an acute infectious disease of the central nervous system caused by clostridium tetani and is characterized by spasms of the skeletal muscles frequently attacking the muscles of the jaw.
Tetanus is commonly known as ‘Lock-jaw.’
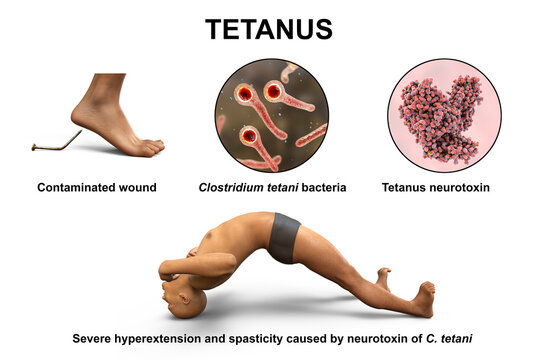
Tetanus is a severe bacterial infection characterized by intermittent spasms (twitching) of voluntary muscles.
It is caused by the neurotoxin tetanospasmin produced by Clostridium tetani, an anaerobic bacterium commonly found in soil, dust, and animal feces. The incubation period ranges from a few days to several weeks (averaging 7-10 days), with shorter periods indicating a more severe infection.
Causative Agent and Transmission:
Tetanus is caused by the exotoxins of clostridium tetani.
The causative agent is Clostridium tetani, whose spores enter the body through various routes:
Deep penetrating wounds: Puncture wounds, lacerations, burns, and crush injuries provide anaerobic conditions ideal for spore germination.
Umbilical cord: In newborns (neonatal tetanus), infection often arises from an unsterile umbilical cord stump.
Other routes: Ear infections, wounds sustained during delivery, and septic abortions can also serve as entry points.
The organism can live for a long time in any condition, especially dirty environments. So it can be found in dust, soil, or grass.
The clostridia can be normal organisms in the alimentary canal of animals but when passed out and gain entry to the human body, they become harmful. The organism can be found in cows, horse, sheep, or goat.
Incidence of tetanus:
In babies born at home before arrival at the hospital.
In homes where domestic animals are kept.
Pathophysiology of Tetanus
The pathophysiology of tetanus involves the invasion of the body by bacilli or spores, typically through deep puncture wounds or cuts. These bacilli find a suitable environment to multiply in anaerobic conditions. It is crucial to note that all unclean wounds pose a significant risk. Once the clostridium tetani organisms enter the wound, they unleash two forms of exotoxins into the surrounding tissues: tetanospasmin and tetanolysin.
Tetanospasmin, a potent toxin, plays a critical role in producing the disease’s clinical manifestations. It primarily affects the central nervous system (CNS). The toxins specifically target the motor nerve cells of the spinal cord and the brain. As a result, spasms develop in the muscles that are supplied by the corresponding nerves.
Route of entry
The route of entry for the clostridium tetani organisms includes various pathways, all of which can lead to infection and subsequent tetanus:
Infected ulcerated wound.
Postoperative wounds.
Umbilical stumps (in newborns).
Gun-shot wounds.
Septic abortion.
Jiggers or foreign bodies.
Burns and scalds.
Clinical Features of Tetanus:
Symptoms typically begin with localized muscle stiffness, progressing to more generalized manifestations:
Trismus (Lockjaw): Difficulty opening the mouth due to masseter muscle spasm. Stiffness of the muscles, particularly noticeable in the jaw. Spasms affecting the muscles of the face, especially the cheek and jaw, leading to difficulty in opening the mouth, a condition referred to as trismus.
Risus sardonicus: A characteristic grimace with a sardonic smile. The angles of the mouth are pulled outwards, causing a forced smile known as risus sardonicus or the “Devil’s grin.”
Dysphagia: Difficulty swallowing. Swallowing becomes challenging as the muscles of the mouth and esophagus are affected by spasms.
Weight loss may occur due to difficulties in eating, leading to starvation.
Muscle spasms: Severe, painful spasms initially affecting the jaw and neck, then spreading to other muscle groups. Spasms can be triggered by stimuli such as sounds or light.
Opisthotonos: Severe arching of the back due to muscle spasms, while the patient remains conscious. The head is thrown back, and the back becomes arched due to the rigid muscles in the neck, a condition called opisthotonus.
Fever: Often present. Patients may experience an elevated temperature and rapid pulse.
Signs of inflammation may be evident, such as swelling of the umbilical cord (if present in newborns), a wet cord, offensive smell, or pus discharge from the wound site.
Respiratory distress: Spasms of respiratory muscles can cause respiratory failure, a life-threatening complication. Spasms affecting the respiratory muscles may lead to prolonged periods without oxygen (anoxia), which can be life-threatening and result in death.
Autonomic nervous system instability: This can lead to fluctuating blood pressure, sweating, and tachycardia.
Hyperreflexia: Exaggerated reflexes.
Absence of a visible wound: Does not exclude a diagnosis of tetanus; infection can sometimes occur without a readily apparent wound.
Spasms of the sphincters can result in retention of urine or stool, and in severe cases, sphincter rupture may occur.
Patients may have a wound or a history of a wound, which could be the point of entry for the tetanus-causing bacteria.
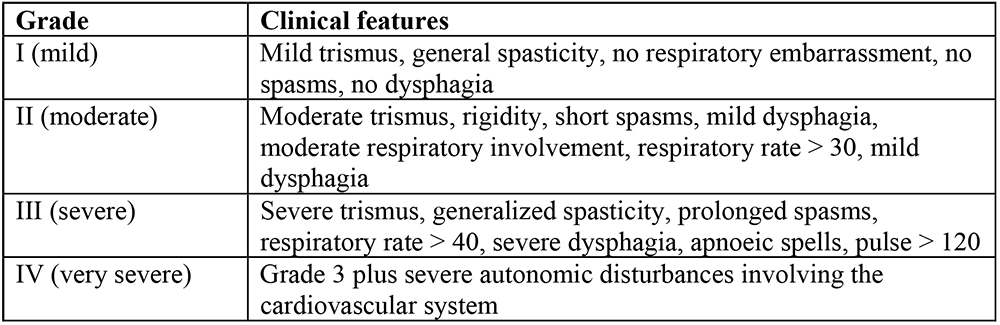
Alblett Classification of Tetanus
There are several grading systems; the scale proposed by Ablett5 is the most widely used . This categorizes patients into four grades depending upon the intensity of spasms, and respiratory and autonomic involvement.
Management of Tetanus
There’s no cure for tetanus. A tetanus infection requires emergency and long-term supportive care while the disease runs its course.
Aims of Management
To control spasms.
To eliminate the causative organism and its toxins.
To prevent complications, and ensure adequate nutrition for the patient.
Specific treatment measures include:
Penicillin: Administering penicillin is a crucial step in destroying the tetanus-causing organism.
Anti-tetanus serum: The administration of anti-tetanus serum helps neutralize the spreading toxins and halt their further detrimental effects.
Sedation and muscle relaxants: Medications like diazepam and chlorpromazine are given to provide sedation and muscle relaxation, effectively alleviating spasms and minimizing discomfort.
Wound management: If there is a wound or focus of infection where the tetanus bacteria may have entered, the dead tissue is excised, and the area is irrigated with hydrogen peroxide. Leaving the wound open without suturing promotes oxygen exposure, hindering the growth of tetanus bacilli, which thrive in anaerobic conditions.
Neutralizing the Toxin:
Tetanus Immunoglobulin (TIG): Human TIG is administered to neutralize circulating toxins. The dose varies depending on age and the severity of the contamination:
Adults and children: 150 IU/kg (administered at least in two different IM sites, separate from the tetanus toxoid injection site).
Neonates: 500 IU IM (in at least two different IM sites).
Tetanus Toxoid (TT) or DPT: The appropriate vaccine (TT or DPT) should be administered immediately to provide active immunity. Refer to the vaccination guidelines for specific age-appropriate regimens.
Eliminating the Source of Toxin:
Wound management: Thorough cleaning and debridement of wounds to remove necrotic tissue and eliminate the bacterial source. For umbilical wounds in neonatal tetanus, meticulous cleaning and debridement of the umbilical stump are essential.
Antibiotic Treatment:
First-line: Metronidazole (500 mg every 8 hours IV or orally for 7 days; children: 7.5 mg/kg every 8 hours).
Second-line: Benzylpenicillin (2.5 MU every 6 hours for 10 days; children: 50,000-100,000 IU/kg per dose; Neonates: 100,000 IU/kg every 12 hours for 10-14 days)
Control of Muscle Spasms:
First-line: Diazepam (10 mg IV or rectal every 1-4 hours; children: 0.2 mg/kg IV or 0.5 mg/kg rectal every 1-4 hours, max 10mg). For Neonates: 0.2 mg/kg IV or 0.5 mg/kg rectal every 1 to 4 hours.
Other agents: Magnesium sulfate (alone or with diazepam), chlorpromazine (alone or alternating with diazepam). Monitor for side effects (e.g., respiratory depression with diazepam, loss of knee-jerk reflex with magnesium sulfate). Chlorpromazine dosage for neonates: 1 mg/kg orally 8 hourly via NGT.
Pain Control:
Morphine: (2.5-10 mg IV every 4-6 hours; monitor for respiratory depression; children: 0.1 mg/kg per dose).
Paracetamol: (1 g every 8 hours; children: 10 mg/kg every 6 hours).
Prevention:
Routine childhood immunization: All children should receive the recommended tetanus toxoid-containing vaccines (DTP, Tdap, or Td) as per national immunization schedules.
Proper wound care: Prompt and appropriate treatment of wounds, including cleaning and debridement, significantly reduces the risk.
Prophylactic TIG: For individuals with contaminated wounds and incomplete or unknown immunization status:
Children < 5 years: 75 IU
Children 5-10 years: 125 IU
Children > 10 years and adults: 250 IU
Wound care: Proper care of wounds, including thorough cleaning and debridement, helps prevent infection.
Control of spasms involves the following measures:
Absolute rest and isolation: The patient should be kept in a quiet room with dim lighting to minimize triggers for spasms.
Prevention of external stimuli: Measures such as fitting the door with suitable closing materials or springs prevent slamming noises that could stimulate the patient.
Warming hands before touching: Nurses should warm their hands before touching the patient to avoid any stimulation that might trigger spasms.
Medication administration: Sedatives and muscle relaxants, such as chlorpromazine (Largactil), and Diazepam, are given regularly through a nasogastric tube to maintain a controlled state and alleviate spasms.
o Example of 6 hourly regimen
Drug
6-9
am
9-12
pm
12-3
pm
3-6
pm
6-9
pm
9-12
am
12-3
am
3-6
am
6-9
am
Largactil
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
Diazepam
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
General Management:
Close observation and airway management: Monitor the patient closely, ensuring a clear airway and using a mucous extractor if necessary.
Vital signs monitoring: Regularly check temperature, pulse, and respirations, noting the severity of the condition. Record the strength, frequency, duration, and body part involved in spasms using a spasm chart.
Nutrition: Maintain adequate nutrition through nasogastric tube feeding to avoid stimulating spasms with injections. Prevent aspiration of fluids into the airway.
Catheterization: Catheterize the patient to maintain proper bladder function.
Fluid balance chart: Monitor and maintain fluid balance, initially using intravenous fluids if necessary and later transitioning to nasogastric tube feeding.
Hygiene: Ensure daily cleaning of the cord with normal saline and perform oral care carefully. Turn the patient every two hours to prevent pressure sores.
Vaccination: Prevent future tetanus cases by ensuring all individuals receive a full course of DPT (diphtheria, pertussis, and tetanus) vaccination.
Use sterile equipment: Prevent cross-infection by using sterile equipment during medical procedures.
Bowel and bladder care: Monitor and assist the patient in passing stool and urine.
Medication: Administer prescribed drugs as instructed.
Physiotherapy: Implement physiotherapy sessions for deep breathing exercises and active limb movements.
Prevention:
Public health education: Raise awareness about the dangers of using unsterilized equipment during childbirth and applying native medicine or other substances to the umbilical cord.
Immunization: Ensure that all women of childbearing age are vaccinated against tetanus.
Safe childbirth practices: Promote safe and clean practices during childbirth to prevent infections.
Discourage harmful practices: Discourage practices like applying cow dung to a child’s umbilical cord.
Wound care education: Educate people on cleaning wounds thoroughly with water and soap to prevent infections. Encourage covering wounds with sterile dressings and seeking early medical attention for cut wounds.
Protective gear: Encourage the use of gum boots when digging to prevent soil-related infections.
Complications of Tetanus
Fracture of bones or the spine: The intense and frequent muscle spasms can cause fractures in bones or the spine, especially if the spasms are severe and uncontrolled.
Pneumonia: Heavy sedation, a common treatment for managing tetanus spasms, may lead to shallow breathing or difficulty in clearing the airway, increasing the risk of pneumonia, a potentially severe respiratory infection.
Brain damage: The potent toxins produced by the tetanus-causing bacteria can affect the central nervous system, leading to brain damage in severe cases.
Growth retardation: In children affected by tetanus, the disease can interfere with proper nutrition and growth, potentially causing growth retardation.
Exhaustion: The continuous and strenuous muscle spasms can lead to extreme exhaustion, further weakening the patient’s overall condition.
Respiratory failure: In severe cases, the spasms can affect the respiratory muscles, resulting in respiratory failure, where the patient is unable to breathe adequately on their own.
Retention of urine: Spasms in the pelvic region can cause the sphincters to contract, leading to difficulty in passing urine and possible urine retention.
Death due to airway obstruction: In the most severe cases, the intense spasms, particularly those affecting the muscles of the jaw and neck, can obstruct the airway, leading to suffocation and potential death.
Quick Quiz
Tetanus Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Overview:Leprosy, historically known as Hansen’s disease, is a chronic, slowly progressing bacterial infection that primarily attacks the skin and the peripheral nerves. According to the Uganda National Tuberculosis and Leprosy Strategy (2025/26–2029/30), Leprosy remains endemic in specific hotspots like the West Nile Region. The modern clinical focus is on very early detection, immediate Multi-Drug Therapy (MDT), aggressive contact tracing, and preventing permanent nerve damage or Grade 2 Disabilities (G2D).
1. Aetiology, Transmission, and Incubation
Cause of Leprosy (Aetiology)
Leprosy is caused by two specific types of bacteria:
Mycobacterium leprae: The traditional, well-known bacillus responsible for the vast majority of leprosy cases globally.
Mycobacterium lepromatosis: A relatively newly identified mycobacterium that was first isolated from a fatal case of diffuse lepromatous leprosy in 2008.
These bacteria are "acid-fast" and strongly prefer the cooler parts of the human body, which is why the disease heavily damages the skin, peripheral nerves near the body surface, the eyes, and the lining of the nose.
Transmission (Mode of Spread)
Leprosy is not highly contagious. It requires prolonged, close contact with an untreated infected person. The main routes of transmission include:
Nasal Route (Droplet Infection): The bacteria are primarily spread through the air via infected nasal secretions when an untreated person sneezes or coughs.
Transplacental: Transmission from an infected mother to her unborn baby across the placenta (rare but possible).
Breast Feeding: Prolonged, close physical contact and transmission via breast milk.
Genetic Predisposition: Modern science shows that over 95% of people are naturally immune to leprosy. However, certain individuals have a genetic weakness in their immune system that makes them highly susceptible to catching the disease when exposed.
Incubation Period
The incubation period refers to the time between when a person is first exposed to the bacteria and when the first signs of the disease actually appear on the body.
The bacteria multiply exceptionally slowly.
The standard incubation period usually lasts from 2 to 5 years.
In severe cases, especially in Lepromatous leprosy, the bacteria can hide and grow for a much longer duration, taking anywhere from 8 to 12 years before obvious signs become apparent.
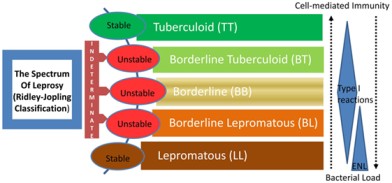
2. Types and Classification of Leprosy
Leprosy presents differently depending entirely on how strong the patient's cellular immune system is.
1. Lepromatous Leprosy (90% of cases):
This is the most common, severe, and highly infectious type. The patient has a very weak cellular immune response. Because the immune system cannot fight back, the bacteria multiply profusely all over the body. This leads to massive, widespread skin lesions and severe, permanent nerve damage. (In Uganda, 86% of new cases are this highly infectious 'multibacillary' type).
2. Tuberculoid Leprosy:
In this type, the patient has a much stronger immune response. The body fights the bacteria well, resulting in only a few, well-defined skin lesions. The affected skin patches may lose sensation, but the overall nerve damage is mild and much less severe compared to the lepromatous type.
3. Borderline Leprosy:
This type lies exactly in the middle between lepromatous and tuberculoid leprosy. The immune response is moderate. It displays mixed characteristics, showing a moderate number of skin lesions and moderate nerve involvement. If untreated, it can quickly downgrade into severe lepromatous leprosy.
4. Undeterminate (Dismorphoid) Leprosy:
This type is diagnosed in the very early stages of the disease when symptoms and the immune response are not yet well-defined. It is difficult to classify precisely. Over time, it will either heal on its own or develop into one of the major types listed above.
Clinical Differences Between the Major Types
Cutaneous (Skin) Feature
Tuberculoid Leprosy
Borderline Leprosy
Lepromatous Leprosy
Number of Lesions
Very Few
Many
Many (Widespread)
Size of Lesion
Large
Both Large and Small
Small
Symmetry of Lesions
Asymmetrical (One side only)
Symmetrical (Both sides)
Symmetrical (Both sides)
Surface of Lesions
Rough and Scaly
Rough and Scaly
Smooth and Shiny
Edges of Lesions
Sharp and clear
Sharp
Vague and poorly defined
3. Clinical Signs and Symptoms
Leprosy presents with a wide variety of signs that destroy both the patient's physical appearance and nervous system.
Anaesthetic Skin Lesions: Patches of skin that completely lose their ability to feel sensation. The patient cannot detect pain, heat, cold, or light touch in these areas. Because they feel no pain, they frequently burn or cut themselves without noticing, leading to severe injuries.
Thickened Peripheral Nerves: The bacteria invade the nerves, causing them to swell and become painfully thick. The midwife can easily feel these enlarged nerves as hard lumps under the skin (especially around the elbows and knees).
Nasal Stuffiness: The bacteria attack the cool lining of the nose, causing chronic inflammation, swelling, and severe congestion.
Saddled Nose: In advanced untreated cases, the bacteria completely eat away and destroy the cartilage inside the nose (nasal septum), causing the entire bridge of the nose to collapse flat.
Loss of Eyebrows and Lashes: The disease destroys the hair follicles on the face, causing a complete loss of eyebrows and eyelashes (a condition medically known as Madarosis).
Erythema Nodosum: Painful, red, raised nodules that erupt on the surface of the skin or deep under the skin's surface, usually during an immune reaction.
Inflammatory Eye Changes: Leprosy attacks the facial nerves that control blinking. The eyes dry out, become inflamed, and develop ulcers, frequently leading to permanent vision impairment or blindness.
4. Investigations and Diagnosis
To officially diagnose leprosy and confirm the presence of the bacteria, healthcare professionals conduct several specific tests:
Skin Snip / Slit-Skin Smear: A very small cut is made in the affected skin (usually the earlobe or lesion edge). The tissue fluid is smeared on a slide and stained using the modified Ziehl-Neelsen (ZN) method to visually identify the bacteria under a microscope.
Polymerase Chain Reaction (PCR): An advanced molecular technique used to detect the exact genetic material (DNA) of the leprosy bacteria in skin samples. It is highly accurate and aids in very early diagnosis.
Histamine Test: A drop of histamine is injected into the skin. A normal person will develop a bright red flare around the injection. In a leprosy patient, because the nerves are dead, there is no red flare. This test proves severe nerve damage.
Lepromin Test: A substance derived from dead leprosy bacteria is injected under the skin. It measures how strongly the body's immune system reacts. It is not used to *diagnose* leprosy, but rather to determine the *type* of leprosy (e.g., Tuberculoid patients react strongly; Lepromatous patients have no reaction because their immunity is too weak).
🔍 National Strategy Focus: Early Case Finding
The Uganda Ministry of Health emphasizes aggressive Active Case Finding (ACF) to diagnose patients early. This involves house-to-house screening, school-based leprosy campaigns, and contact tracing. The goal is to catch the disease before it causes Grade 2 Disability (visible deformities), which is currently alarmingly high at 24% of new diagnoses.
5. Treatment and Management of Leprosy
Leprosy is 100% curable. Treatment relies heavily on Multi-Drug Therapy (MDT) to kill the bacteria completely and prevent them from developing drug resistance.
Primary MDT Drugs Used
Leprosy Classification
Drug Combination Regimen
Tuberculoid Leprosy
Dapsone + Rifampicin (Usually taken for 6 months).
Borderline Leprosy
Dapsone (Often combined with Rifampicin depending on severity).
Lepromatous Leprosy
Dapsone + Rifampicin + Clofazimine (Taken for a minimum of 12 months, sometimes longer, to clear the massive bacterial load).
Non-Leprosy Drugs Used in Management
Steroids (e.g., Prednisolone): Used aggressively to calm down severe immune reactions and reduce inflammation around the nerves (neuritis), preventing permanent paralysis.
Vitamin B Complex: Given routinely to nourish, protect, and promote the healing of damaged peripheral nerves.
Leprosy Prevention (National Guidelines)
SDR-PEP (Single-Dose Rifampicin Post-Exposure Prophylaxis): Uganda's current strategy mandates tracing every person living in the same house as a leprosy patient. After checking them to ensure they don't already have the disease, they are given a single large dose of Rifampicin to kill any hiding bacteria and prevent them from ever falling sick.
Visual representation of advanced leprosy complications including Leonine facies, claw hands, and collapsed nasal bridge.
6. Severe Complications of Leprosy
If diagnosis is delayed or treatment is not completed, the continuous nerve and skin damage leads to catastrophic, lifelong deformities. These include:
Madarosis: The complete, permanent loss of eyebrows and eyelashes.
Nasal Bridge Collapse: The "Saddle Nose" deformity resulting from the destruction of facial cartilage.
Leonine Facies: The skin on the face becomes massively thickened, folded, and lumpy, giving the patient a frightening, lion-like facial appearance.
Elongated Soft Ear Lobes: The earlobes swell with bacteria, becoming heavy, droopy, and permanently stretched.
Ocular Complications: Paralysis of the eyelids means the eyes cannot close or blink. Dust and dryness cause severe corneal ulcers and eventual permanent blindness.
Loss of Sensation: Total loss of the ability to feel heat, sharp pain, or light touch on the hands and feet.
Multiple Ulcerations: Because the patient feels no pain, they repeatedly burn themselves on cooking fires or cut their feet on stones. These injuries become infected, forming deep, rotting ulcers.
Nerve Enlargement: Hard, painful swelling of major peripheral nerves.
Contractures & Shortening of Phalanges: The muscles in the hands become paralyzed and shrink. The fingers (especially the 4th and 5th fingers) curl into a rigid "claw hand." Over time, the bone tissue is reabsorbed by the body, making the fingers and toes incredibly short and stubby.
Hammer Toes: Abnormal, rigid bending of the toe joints caused by muscle paralysis in the foot.
Disuse Atrophy: Severe wasting and shrinking of muscles in different parts of the body because paralyzed limbs cannot be used.
Orchitis: Severe, painful inflammation of the testicles as bacteria invade the reproductive organs.
Sterility in Men: The secondary result of prolonged orchitis, permanently destroying the man's ability to produce sperm.
Reactional States (Erythema Nodosum Leprosum): Ironically, when drug therapy successfully starts killing the bacteria, the immune system can suddenly overreact to the dead bacterial bodies. This causes massive fevers, nerve pain, and painful red skin lumps. It is an emergency requiring immediate steroids to save the nerves.
📝 Quick Clinical Review
Scenario: A patient is diagnosed with Lepromatous leprosy. Why are they at a much higher risk of developing deep foot ulcers compared to someone with Tuberculoid leprosy?
Answer: Lepromatous leprosy involves massive, widespread bacterial growth due to a weak immune response. This results in severe, widespread destruction of the peripheral nerves. The patient completely loses pain sensation in their feet, meaning they will repeatedly step on sharp objects or walk on injured feet without knowing, leading to massive, deep, painless ulcers.
Quick Quiz
Leprosy Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
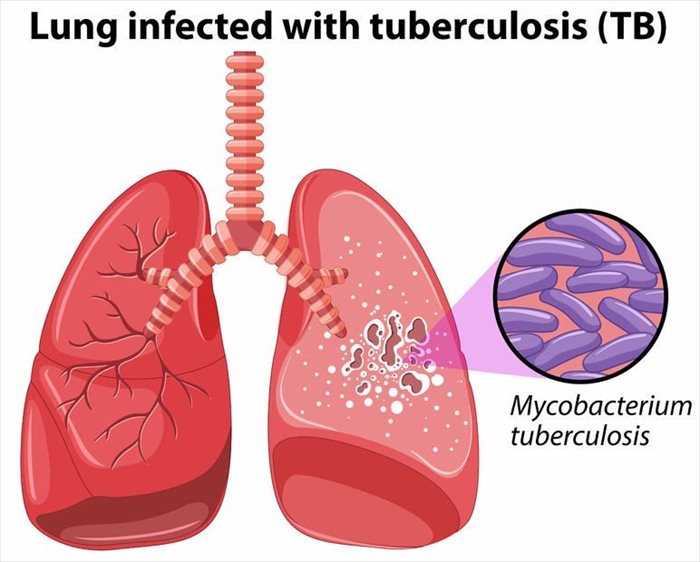
Tuberculosis (TB) & New National Management Guidelines
Overview:Tuberculosis (TB) is a highly infectious, widespread, and often deadly disease caused by strains of mycobacteria. While it primarily attacks the respiratory system (lungs), it can aggressively spread to any organ in the body. According to the updated Uganda National Tuberculosis and Leprosy Strategy (2025/26–2029/30), TB remains a massive public health emergency, with a high burden of TB/HIV co-infection, childhood TB, and emerging Drug-Resistant TB (DR-TB). The goal is to aggressively scale up rapid molecular diagnostics, shorter treatment regimens, and community-led digital monitoring to End TB.
1. Aetiology and Mode of Spread
Aetiology (Cause of the Disease)
The primary causative organism for this disease is Mycobacterium tuberculosis (also known as the Tubercle Bacillus). It is a small, aerobic (requires oxygen to survive), non-motile (cannot move on its own) bacillus (rod-shaped bacterium).
Mode of Spread (Transmission)
Tuberculosis is highly contagious and spreads through multiple pathways:
Airborne Droplet Infection: The bacteria spread rapidly through the air when an individual with an active, untreated pulmonary TB infection coughs, sneezes, speaks, or sings. This releases invisible respiratory fluids containing the bacilli into the air.
Haematogenous Spread: Once inside the body, the bacteria can enter the bloodstream and spread to distant organs.
Close Contact: Prolonged, frequent, or intense contact with a person who has infectious TB (such as living together or spending a great deal of time in close proximity).
Zoonotic TB: Though less common today, Mycobacterium bovis can be transmitted through consuming unpasteurized milk or direct contact with infected cattle/abattoir environments.
2. Classification and Types of Tuberculosis
Tuberculosis is broadly classified based on the site of infection, the patient's exposure history, and its resistance to medications:
Pulmonary Tuberculosis (PTB): TB strictly affecting the lungs. It is the most common and the only highly infectious form.
Extra-Pulmonary Tuberculosis (EPTB): TB affecting organs outside the lungs (e.g., bones, brain, lymph nodes). It is generally not infectious to others.
Primary Tuberculosis: The very first time a person is exposed to and infected with the TB bacteria.
Secondary Tuberculosis: A reactivation of a dormant TB infection or a massive new reinfection from the environment.
Latent TB Infection (LTBI): The bacteria are alive but inactive (sleeping) inside the body. The patient has no symptoms, does not feel sick, cannot spread the disease, but tests positive on skin or blood tests.
Drug-Resistant TB (DR-TB) Classifications
According to WHO and National Guidelines, DR-TB occurs when bacteria survive despite the use of standard medicines. It is classified as:
Mono-resistant TB: Resistance to exactly one first-line anti-TB drug.
Poly-resistant TB: Resistance to more than one first-line drug (but NOT both Isoniazid and Rifampicin together).
Rifampicin-Resistant TB (RR-TB): Resistance specifically to Rifampicin, detected with or without resistance to other drugs. Treated identically to MDR-TB.
Multidrug-Resistant TB (MDR-TB): Resistance to at least both Isoniazid and Rifampicin, the two most powerful first-line drugs.
Extensively Drug-Resistant TB (XDR-TB): MDR-TB plus additional resistance to any Fluoroquinolone and at least one Group A drug (like Bedaquiline or Linezolid).
3. Clinical Features (Signs and Symptoms)
A. Pulmonary TB
Patients with active lung TB classically present with:
Persistent Cough: Lasting for more than 2 to 3 weeks. It may be productive (with thick sputum) or a non-productive, dry cough.
Haemoptysis: Coughing up fresh blood or blood-stained sputum due to severe lung tissue destruction.
Fever and Chills: Usually a low-grade fever that peaks in the late afternoon or evening.
Night Sweats: Profuse, drenching sweating during sleep.
Weight Loss & Anorexia: Severe loss of appetite resulting in noticeable, unexplained body wasting.
Easy Fatigability: Extreme weakness and lack of energy.
Chest Pain: Pain while breathing or coughing due to pleural involvement.
Finger Clubbing: Abnormal swelling and rounding of the fingertips, caused by chronic lack of oxygen (hypoxia) over a long period.
B. Extra-Pulmonary TB (EPTB)
In approximately 15-20% of active cases (and over 50% in HIV+ patients), the bacilli escape the lungs. Notable sites include:
The Pleura: Causes Tuberculous Pleurisy (fluid and inflammation around the lungs).
Central Nervous System (CNS): Causes Tuberculous Meningitis, a highly fatal swelling of the brain lining.
Lymphatic System: Causes swollen, matted TB lymph nodes (often in the neck, historically called Scrofula).
Genitourinary System: Causes Urogenital Tuberculosis, affecting the kidneys and reproductive organs.
Bones and Joints: Known as Osseous Tuberculosis or TB Osteomyelitis. When it destroys the spine, it is called Pott’s Disease.
Skin: A deep tubercular abscess can burst through the skin, forming a painless, discharging Tuberculous Ulcer.
⚠️ Clinical Alert: Miliary Tuberculosis
This is a severe, widespread, and life-threatening form of TB. It happens when massive amounts of bacteria enter the bloodstream and spread everywhere, forming tiny "millet-seed" sized white spots all over the body's internal organs. Miliary TB accounts for about 10% of extra-pulmonary cases and is highly common in young children and immunocompromised patients.
4. Epidemiology and High-Risk Populations (Uganda Context)
Epidemiology (2024/2025 Data)
Global: Approximately one-third of the global population is infected with dormant TB. Africa has the world's highest incidence rate.
Uganda Incidence: Uganda is among the 30 high TB and TB/HIV burden countries globally. The incidence is 198 cases per 100,000 population, equating to about 96,000 new cases annually.
Missed Cases: Despite progress, approximately 20,000 TB cases remain undiagnosed annually in Uganda.
Demographics: Men account for ~64% of cases. Children (0-14 years) account for 13.8% of notifications.
Co-infection & Mortality: The TB/HIV co-infection rate is dangerously high at 37%. TB causes roughly 15,000 deaths annually in Uganda.
High-Risk and Vulnerable Populations
Uganda's National Strategy heavily prioritizes active case finding in the following groups:
People in Prisons: Prevalence is alarmingly high at 1,904 per 100,000 (nearly 8 times the national average), heavily driven by overcrowding and poor ventilation.
People Living with HIV (PLHIV): HIV is the most significant global risk factor, weakening the immune system and driving the rapid progression of active TB.
Children under 5 & Adolescents: Highly vulnerable to severe forms like meningitis and miliary TB. Contact tracing is crucial.
Men: Men have a higher prevalence but poor health-seeking behavior, leaving many undiagnosed and untreated.
Other Key Populations: Urban slum dwellers, miners, pastoralists, refugees, healthcare workers, tobacco smokers, and people with diabetes or severe undernutrition.
5. Pathogenesis: The Cellular Process
Primary Tuberculosis
The bacilli are inhaled deep into the lung air sacs (alveoli), where they invade macrophages, replicate, and trigger an inflammatory response.
They travel through the lymphatic system to the hilar lymph nodes (nodes in the center of the chest).
About 6 weeks after infection, the body’s immune system wakes up. The bacilli are surrounded and "walled off" by specialized immune cells (macrophages, T and B lymphocytes, fibroblasts, and epithelioid cells).
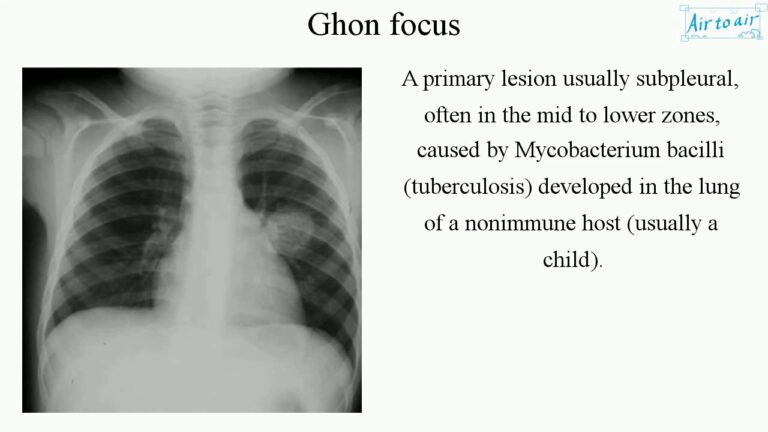
This hard, trapped nodule in the lung is called a Ghon Focus.
The combination of the Ghon Focus and the swollen hilar lymph nodes is called the Primary Complex.
In 90% of people, the bacteria stay asleep inside this wall for years (Latent TB).
Diagram illustrating the formation of a Ghon Focus and the Primary Complex within the lungs.
Secondary Tuberculosis & Caseation
Occurs due to reactivation of dormant bacilli (when immunity drops) or massive reinfection.
Inside the immune walls (Granulomas), abnormal cell death occurs. The center turns into a soft, white, cheese-like substance. This is called Caseation Necrosis.
Tissue destruction and necrosis are balanced by healing and fibrosis. If the bacteria win, they dissolve the lung tissue, leaving large empty holes called Cavities filled with highly infectious caseous material.
6. Diagnosis and Investigations (Modern Guidelines)
Uganda's current standard of care has aggressively shifted away from basic microscopy towards Universal access to Molecular WHO-Recommended Rapid Diagnostics (mWRDs).
Diagnostic Tool
Clinical Application & Modern Strategy
GeneXpert / TrueNat (mWRDs)
The absolute first-line test. GeneXpert Ultra machines rapidly detect both the TB DNA and Rifampicin resistance (RR-TB) simultaneously. The goal is 100% molecular testing.
Digital Chest X-Ray (dCXR) with CAD/AI
Used heavily for screening, especially in mobile vans and high-risk populations. Computer-Aided Detection (CAD) Artificial Intelligence helps automatically flag abnormal infiltrates, cavities, or nodules.
Urine LF-LAM
A specialized rapid test using urine. Highly effective and specifically indicated for screening TB in PLHIV with advanced disease (very low CD4 counts).
Stool Testing
An alternative specimen collection method now recommended for Childhood TB, as children swallow their sputum and cannot expectorate easily.
Culture & Second-Line DST
Samples are referred to the National TB Reference Laboratory (NTRL) to grow the bacteria and perform comprehensive Drug Susceptibility Testing (DST), including Line Probe Assays (LPAs) and Next Generation Sequencing (NGS) for MDR/XDR-TB.
Sputum Microscopy (AFB)
Still available but now primarily used for treatment follow-up to see if the patient is converting to negative, rather than initial diagnosis.
Tuberculin Skin Test (Mantoux)
Used to assess Latent TB Infection (LTBI), especially in children and healthcare workers.
7. The Relationship Between HIV and TB Co-Infection
HIV and Tuberculosis are deeply connected. They act together in a deadly cycle where each disease makes the other much worse. Understanding their relationship is critical for a midwife managing infectious diseases.
A. Effects of HIV on Tuberculosis
HIV severely weakens the immune system (destroying CD4 cells), which changes how TB behaves in the body:
Development of active TB: Individuals infected with HIV have a much higher risk of developing active tuberculosis once they are exposed to the TB bacteria, instead of keeping it dormant.
High risk of re-infection: HIV-positive individuals are highly susceptible to being infected with a brand new, second strain of TB from the environment, even after they have already had the infection and been treated.
Increased incidence of TB: The overall number of tuberculosis cases in the population increases greatly due to the high prevalence of HIV, which weakens the community's immune defenses and makes individuals far more susceptible to catching TB.
Changes in TB presentation: TB in HIV-positive individuals often presents with completely different clinical and bacteriological signs. Because the immune system cannot form cavities to fight the bacteria, patients may have a non-productive (dry) cough, a total absence of hemoptysis (no coughing up blood), and X-rays will show a scattered miliary pattern instead of the typical large lung cavitations.
Quicker development of TB complications: HIV acts as an accelerator, speeding up the progression of TB disease and causing severe complications much faster than in an HIV-negative person.
B. Effects of Tuberculosis on HIV
Increased HIV replication: TB infection causes massive inflammation in the body. This immune response actually enhances and speeds up the replication of the HIV virus, leading to a much higher viral load and a faster progression into full-blown AIDS.
Common opportunistic infection: TB is one of the most frequent opportunistic infections to attack individuals living with HIV. It stands as the leading cause of death in this vulnerable population.
Interference with ARV treatment: Strong anti-TB medications, specifically Rifampicin, can heavily interfere with certain antiretroviral drugs (ARVs), such as Nevirapine and Protease Inhibitors. This dangerous drug-to-drug interaction necessitates expert adjustments in the patient's treatment plan.
C. Consequences of Dual Infection (Having both HIV and TB)
Increased morbidity and mortality: Patients suffer much higher rates of severe sickness and death.
Higher recurrence rate: There is a higher chance of the TB coming back even after successfully completing a full course of treatment.
Drug resistance: Dual infection often leads to poor drug absorption and resistance, resulting in dangerous Multidrug-Resistant TB (MDR-TB) and Extensively Drug-Resistant TB (XDR-TB).
Higher rates of treatment non-adherence: Because the patient has to swallow so many pills for both HIV and TB (overlapping medication regimens), they often get tired and stop taking their drugs.
Increased risk of drug toxicity: Taking strong TB drugs and ARVs at the same time heavily stresses the liver and kidneys, leading to severe toxic side effects.
⚠️ Management of HIV and TB Co-infection
When a patient has both diseases, the timing and management of their medications must follow strict clinical guidelines:
Prioritize TB Treatment First: Always start treating the Tuberculosis before starting the ARVs to prevent deadly immune reactions.
Timing of ARVs: Start ARVs if the patient's CD4 count is below 350 cells/mm³. This is usually done either immediately after finishing TB treatment or carefully during the intensive phase of TB treatment, depending on the patient's exact clinical situation.
Manage Drug Interactions: Carefully consider the chemical interactions between TB drugs (like Rifampicin) and HIV regimens when selecting the final medications.
Use DOTS: Strictly use Directly Observed Therapy (DOTS) for the TB treatment and monitor the patient very closely for signs of organ toxicity and to ensure absolute adherence.
Administer Prophylaxis: Give prophylactic drugs (like Cotrimoxazole/Septrin) to prevent other opportunistic infections as indicated.
Complications of Tuberculosis
If TB is not diagnosed early or treated completely, the bacteria will physically destroy the body's tissues, leading to severe, life-threatening complications:
Pleural effusion: The abnormal and dangerous accumulation of fluid in the pleural space (the thin lining surrounding the outside of the lungs), which crushes the lung and makes breathing extremely difficult.
Pericardial effusion: The abnormal accumulation of fluid in the sac surrounding the heart, which squeezes the heart muscle and prevents it from pumping blood properly.
Empyema: The fluid in the pleural space becomes infected and turns into a thick, highly toxic, pus-filled cavity.
Pneumothorax: The TB bacteria eat through the lung tissue, allowing air or gas to leak out into the pleural cavity. The trapped air builds pressure, causing the lung to completely collapse.
Lung fibrosis: Heavy, permanent scarring and stiffening of the delicate lung tissue, leading to permanently impaired lung function and lifelong breathing problems.
Lung collapse: The collapse of an entire lung or just a part (lobe) of a lung due to severe blockage of the airways or compression from outside fluid/air.
Extra-pulmonary TB: The TB bacteria escape the lungs and aggressively attack other vital organs. A prime example is TB Meningitis, where the bacteria attack the lining of the brain and spinal cord, which is frequently fatal.
8. Complications of Untreated TB
Pleural Effusion: A massive accumulation of fluid in the pleural space, crushing the lungs.
Empyema: The fluid in the pleural cavity turns into a thick, toxic pocket of pus.
Pericardial Effusion: Fluid building up in the sac around the heart, restricting its ability to pump.
Pneumothorax: Lung tissue is destroyed, leaking air into the chest cavity and causing lung collapse.
Lung Fibrosis & Post-TB Lung Disease (PTLD): Heavy, permanent scarring of the lung tissue. Uganda guidelines now emphasize assessing Quality of Life post-treatment and linking patients with PTLD to pulmonary rehabilitation.
9. Treatment and Management Guidelines
Aims of TB Treatment
To completely cure the patient (achieve >95% Treatment Success Rate).
To prevent complications, death, and Post-TB disabilities.
To rapidly reduce the transmission of TB to the community.
Standard TB Treatment Regimens (The Shift to Shorter Courses)
Uganda is actively updating regimens based on the latest WHO evidence to improve adherence and reduce patient costs.
Patient Category
Modern Treatment Strategy & Regimen Notes
Drug-Susceptible TB (DS-TB) - Adult
Standard 6-month regimen (2HRZE / 4HR). However, the NSP mandates scaling up and evaluating new shorter 4-month DS-TB regimens to improve completion rates.
Childhood TB (DS-TB)
Scale up the use of shorter child-friendly regimens (4-month regimens) and ensure the uninterrupted supply of optimized pediatric FDCs (Fixed Dose Combinations).
MDR-TB / RR-TB
Aggressive expansion of decentralized care using shorter, all-oral regimens (e.g., BPaLM / BPaL). This avoids painful daily injections, reduces toxicity, and has pushed DR-TB success rates to 88%.
🧠 Memory Trick: The Core First-Line Anti-TB Drugs
Remember the acronym STRIPE:
S - Streptomycin (S)
T - (often substituted or dropped in modern oral regimens, but part of historical first-line)
R - Rifampicin (R)
I - Isoniazid (H or INH)
P - Pyrazinamide (Z)
E - Ethambutol (E)
*Note: Pyridoxine (Vitamin B6) is always co-administered with Isoniazid to prevent peripheral neuropathy (nerve damage). Corticosteroids (Steroids) are added for severe inflammation like TB Meningitis or Pericarditis.
Socio-Economic Support & Catastrophic Costs
A major focus of modern TB management is protecting the patient's finances. Over 53.1% of TB-affected households face catastrophic costs (spending >20% of their annual income on transport, nutrition, and hidden fees). The strategy mandates:
Providing Enabler Packages (food rations, transport vouchers, cash transfers).
Linking patients to social protection schemes (PDM, SAGE).
Removing all patient fees for Chest X-rays in public facilities and reimbursing private facilities to offer them free of charge.
10. DOTS, Digital Health, & Community Prevention
Modernizing DOTS (Directly Observed Therapy)
While traditional DOTS relies on a trained worker physically watching the patient swallow pills, Uganda is rapidly scaling up Digital Adherence Technologies (DATs):
Smart Pill Boxes: Boxes that log exactly when the patient opens them.
Video DOT (VDOT): Patients record themselves taking medication via smartphone, allowing remote monitoring.
DSD Models: Differentiated Service Delivery allows stable patients to receive fast-track community refills rather than traveling long distances to the clinic daily.
Preventive Treatment (TPT) & Contact Tracing
TB Preventive Treatment (TPT): Giving prophylactic drugs (like 1HP, 3HP, 3HR) to high-risk groups to stop Latent TB from becoming active. The target is 95% coverage for children under 5, PLHIV, and household contacts.
Contact Investigation: Systematically tracing, line-listing, and screening every person living in the household of a confirmed TB patient.
Multisectoral Accountability Framework (MAF-TB): Engaging non-health sectors. Examples include the Ministry of Education enforcing school ventilation, Ministry of Internal Affairs screening prisoners, and the Ministry of Transport enforcing ventilation in taxis to prevent airborne spread.
📝 Quick Review
Question: Why is the national strategy heavily pushing for the adoption of Digital Adherence Technologies (DATs) like Video DOT (VDOT) and Smart Pill Boxes?
Answer: Because TB treatment is very long. DATs reduce the catastrophic transport costs for patients who previously had to travel to the clinic daily, while still allowing the midwife/health system to guarantee the patient is taking their medication, preventing drug resistance (MDR-TB).
11. References
World Health Organization (WHO) Guidelines for Treatment of Tuberculosis.
Uganda Ministry of Health (MoH) National Tuberculosis and Leprosy Programme (NTLP) Manual.
UNMEB Curriculum for Diploma in Midwifery/Nursing - Tropical Medicine & Medical Disorders.
Quick Quiz
Tuberculosis Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Measles, also known as Morbilli, is a highly contagious acute infection of the respiratory system caused by the morbillivirus.
It is characterized by a widespread skin rash, fever, and inflammation of the mucous membranes.
Measles, also known as rubeola, is a highly contagious, acute viral infection characterized by a generalized skin rash accompanied by pathognomonic Koplik’s spots.
The transmission of measles occurs through respiration, mainly by coming into contact with fluids from the nose and mouth of an infected person. Due to its high contagion, it can easily spread among individuals.
Aetiology (Cause):
Measles is caused by the measles virus, a single-stranded RNA virus belonging to the genus Morbilliviruswithin the family Paramyxoviridae. The virus is a multi-shaped, spherical structure with a diameter of 100-250 nm. It consists of six proteins, an inner capsid containing a helical strand of RNA, and an outer envelope.
Transmission:
The primary route of transmission is airborne, through inhalation of respiratory droplets expelled by an infected person during coughing, sneezing, or talking. Other transmission routes include:
Ingestion (fecal-oral): Transmission through contaminated food or water containing infected stool.
Direct contact: Contact with infected stool or contaminated objects.
Incubation Period:
The incubation period for measles is usually 10-14 days.
Patients are contagious for 1 to 2 days before the onset of symptoms and remain infectious for up to 4 days after the appearance of the rash. Infectivity peaks during the prodromal phase.
Risk Factors
Several risk factors increase the likelihood of contracting measles, including:
Immunodeficiency in children.
Traveling to regions where measles is common or having contact with individuals who have visited these areas.
Malnutrition, which can weaken the immune system.
Pregnancy, as it may increase susceptibility to the virus.
Vitamin A deficiency, which can compromise the body’s ability to fight infections.
Pathogenesis and Pathology:
After entering the respiratory system, the measles virus infects the respiratory epithelium and spreads via the bloodstream to various organs, including the skin, respiratory tract, and other systems. The virus infects white blood cells, contributing to the establishment of infection.
Generalized Damage: The respiratory system is particularly susceptible to damage, leading to loss of cilia and increasing susceptibility to secondary bacterial infections like pneumonia and otitis media.
Immune Response: The body mounts an immune response, but this can cause inflammation and damage to tissues.
Signs and Symptoms of Measles (Stages):
Measles, an acute and highly communicable infection caused by the morbillivirus, presents a clinical picture that can be divided into three distinct stages: prodromal, eruptive, and convalescent. Suspecting measles becomes crucial when patients exhibit the classic triad of the three “Cs”: cough, conjunctivitis, and coryza.
Stage 1: Prodromal Phase (3 days):
The incubation period lasts approximately 10-14 days.
Patients may not show any signs or symptoms during this stage.
Abrupt onset of mild to moderate symptoms, characterized by:
Fever
Headache
General malaise
Loss of appetite (anorexia)
Enlarged neck lymph nodes
Abdominal pain
Diarrhea
Vomiting
Stage 2: Eruptive Stage(Exanthem (Rash)
Abrupt onset with severe symptoms, including:
Very high fever
Cough
Photophobia (sensitivity to light)
Red eyes and conjunctivitis
Hoarseness of the voice
Distinctive Koplik spots on the mucous membrane of the mouth, next to the molar teeth. These spots may disappear once the rash appears.
Temperature rises on the first day (37.8-39.4 degrees Celsius), may slightly fall on the third day, then rise again on the fourth day with the onset of the rash.
The rash appears around the fourth day and starts on the forehead, behind the ears, neck, and then spreads over the face and entire body. The rash is a red maculo-papular eruption, giving the face a bloated, swollen appearance.
Stage 3: Convalescent Stage
Improvement and disappearance of signs and symptoms begin.
Key features include:
Desquamation of the skin (shedding of the rash)
A decline in body temperature
Resolution of hoarseness of the voice
Weight gain as the patient’s condition improves.
Predisposing Factors:
Unprotected communities with low immunization coverage: Lack of vaccination is a primary risk factor.
Malnourished children: Nutritional deficiencies weaken the immune system.
Overcrowding and poor ventilation: Close contact and enclosed spaces facilitate transmission.
Children with previous severe infections: Prior illnesses, like tuberculosis, can compromise immune function.
Nursing Care/Management for a Patient within 72 Hours of Measles:
Aims of Care/Management:
To reduce body temperature.
To correct dehydration.
To prevent further complications.
Admission:
Admit the child to a well-ventilated room in an isolation unit in the children’s ward.
Record the patient’s particulars, including name, age, next of kin, and full address on the admission forms.
Reassure the mother/caregiver about the child’s condition.
Observations:
Monitor vital signs (Temperature, pulse, respiration, blood pressure, and weight) and record them in an observation chart for baseline monitoring.
Conduct a comprehensive head-to-toe assessment to identify any abnormalities such as jaundice, edema, dehydration, cyanosis, anemia, and lymphadenopathy. Document findings in the patient file.
Inform the doctor about the patient’s condition and prepare for any required investigations and medical treatments.
Carry out procedures, such as tepid sponging, based on the patient’s findings (e.g., in case of high fever).
Investigations:
Conduct necessary investigations to rule out other diseases, such as:
Blood slide for malaria parasites
Full blood count (FBC) to rule out other infections
Urinalysis
Salivary measles-specific IgA testing (rarely done).
Medical Treatments:
There is no specific treatment for measles; it is managed symptomatically.
Prescribe the following drugs based on symptoms:
Antibiotics to treat underlying infections (e.g., Cephalexin or Amoxyl syrup).
Intravenous Ceftriaxone for severe cases.
Analgesics to reduce pain and fever (e.g., Syrup Cetamol).
Antihistamines to reduce itching (e.g., Calamine lotion).
Vitamins A capsules for children below 1 year to prevent eye complications.
Grovit drops or syrup multivitamin to improve appetite.
Fluids and Diet:
Provide plenty of oral fluids to replace lost fluids due to vomiting and diarrhea.
Offer easily digestible foods rich in vitamins and proteins for quick recovery.
Encourage the child to take frequent small meals.
Use a nasogastric tube for feeding if the child cannot eat or drink.
Administer intravenous fluids in cases of severe dehydration.
Skin Care:
Pad the fingers to prevent excessive scratching of the skin.
Apply prescribed calamine lotion to relieve itching.
Mouth and Eye Care:
Emphasize oral hygiene with frequent mouth care using warm saline.
Keep the nostrils clean and maintain cleanliness around the nasogastric tube.
Apply gentian violet 1% for mouth ulcers.
Use glycerin borax to lubricate the lips and prevent cracking.
Clean the eyes with warm saline and avoid rubbing them.
Apply TEO ointment if necessary.
If one eye is affected, encourage the child to lie on the affected side to prevent infecting the other eye.
Avoid direct sunlight on the eyes.
Hygiene and Bed Rest:
Give the patient a daily bath and change bedding frequently.
Use appropriate precautions for discharging ears and administer antibiotics as needed.
Disinfect used soiled linen and utensils.
Properly dispose of used swabs, discharges, or secretions.
Visitor and Ward Management:
Restrict visitors and maintain visiting hours.
Keep radio and TV volumes low to allow for patient rest.
Encourage dim lighting due to photophobia.
Encourage adequate sleep by switching off lights and minimizing noise.
Observations:
Continue monitoring the patient’s general condition and vital signs regularly.
Take note of any deviations from the normal and act accordingly.
Perform tepid sponging, give cold drinks, and apply cold compress on the forehead if the temperature is very high.
Bowel and Bladder Care:
Observe and treat diarrhea or constipation as needed.
Monitor and address any issues with the child’s urine output.
Exercises and Health Education:
Encourage the patient to do active and passive exercises, including deep breathing exercises.
Stimulate the child’s mind with play objects like toys.
Educate the mother/caregiver about the mode of spread, signs, symptoms, and prevention of measles.
Complications of Measles:
Measles can lead to various complications, some of which can be severe and life-threatening, especially in young children and immunocompromised individuals.
Respiratory System:
Laryngitis: Inflammation of the larynx, characterized by hoarseness and difficulty breathing.
Croup: A viral infection affecting the upper airway, resulting in a characteristic barking cough and stridor (a high-pitched whistling sound during breathing).
Bronchitis: Inflammation of the bronchi, causing coughing, wheezing, and difficulty breathing.
Pneumonia: Infection of the lungs, a leading cause of measles-related mortality. This can be caused by either the measles virus itself (primary viral pneumonia) or by secondary bacterial infections.
Bronchiectasis: Permanent widening of the bronchi, leading to chronic coughing and mucus production.
Central Nervous System (CNS):
Encephalitis: Inflammation of the brain, a rare but serious complication.
Mental Retardation: Long-term cognitive impairment, potentially a consequence of encephalitis.
Epilepsy: A neurological disorder characterized by recurrent seizures.
Gastrointestinal (GIT):
Gastroenteritis: Inflammation of the stomach and intestines, causing diarrhoea, vomiting, and abdominal pain.
Hepatitis: Inflammation of the liver, potentially leading to jaundice and liver dysfunction.
Mesenteric Adenitis: Inflammation of the lymph nodes in the mesentery, a fold of tissue that supports the intestines.
Appendicitis: Inflammation of the appendix, requiring surgical intervention.
Ileocolitis: Inflammation of the ileum (lower part of the small intestine) and colon.
Ear, Nose, and Throat (ENT):
Otitis Media: Infection of the middle ear, leading to ear pain, fever, and hearing loss.
Corneal Ulceration: Ulcers on the cornea of the eye, potentially causing vision impairment.
Others/Rare:
Myocarditis: Inflammation of the heart muscle, affecting heart function.
Glomerulonephritis: Inflammation of the kidneys, potentially leading to kidney failure.
Exacerbation of Tuberculosis (TB): Measles can reactivate latent tuberculosis infection due to compromised immunity.
Quick Quiz
Measles Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Malaria is an acute febrile illness caused by the Plasmodium parasite, which invades red blood cells (RBCs).
It is an infectious disease where parasitic protozoa of the genus Plasmodium multiply within RBCs, leading to a variety of clinical manifestations.
Aetiology:
Parasite: The causative agent of malaria is a protozoan parasite belonging to the genus Plasmodium. There are five species that infect humans:
Plasmodium falciparum: The most dangerous species, responsible for the majority of severe and fatal cases.
Plasmodium vivax: Causes benign tertian malaria (fever every 48 hours), but can cause serious complications in some cases.
Plasmodium ovale: Causes ovale malaria, similar to vivax malaria, but is less common.
Plasmodium malariae: Causes quartan malaria (fever every 72 hours). While typically less severe, can lead to chronic complications.
Plasmodium knowlesi: Primarily infects monkeys but can be transmitted to humans.
Vector: The parasite is transmitted to humans through the bite of an infected female Anopheles mosquito, also known as the “malaria mosquito.”
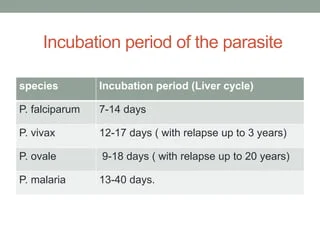
Incubation Period
The period between the mosquito bite and the onset of malarial illness usually ranges from one to three weeks (7 to 21 days).
However, certain types of malaria, such as P. vivax and P. ovale, may take much longer, up to eight to 10 months, to cause symptoms. These parasites remain dormant (inactive or hibernating) in the liver cells during this extended period.
Unfortunately, some dormant parasites may persist even after a patient recovers from malaria, leading to the possibility of relapsing malaria, wherein the patient may fall ill again.
Transmission:
Mosquito Bite: An infected female Anopheles mosquito bites a human and injects sporozoites (infective stage of the parasite) into the bloodstream.
Liver Stage: Sporozoites travel to the liver and invade liver cells, where they multiply asexually.
Blood Stage: After several days, the parasite enters the bloodstream as merozoites, invading red blood cells.
Blood Stage Multiplication: Merozoites multiply asexually within red blood cells, causing their rupture and releasing more merozoites.
Sexual Stage: Some parasites develop into gametocytes, the sexual stage.
Mosquito Ingestion: If a mosquito bites an infected human, it ingests gametocytes.
Mosquito Development: Inside the mosquito, gametocytes mature and fertilize, forming sporozoites.
Mosquito Transmission: The sporozoites migrate to the mosquito’s salivary glands, ready to infect another human.
Predisposing Factors:
Geographic Location: Malaria is endemic in tropical and subtropical regions with suitable mosquito breeding grounds.
Age: Children under five are at the highest risk of severe malaria.
Immune Status: People with weakened immune systems (e.g., due to HIV/AIDS or malnutrition) are more susceptible to severe disease.
Pregnancy: Pregnant women are more vulnerable to malaria, as the parasite can affect both mother and fetus.
Travel History: Travelers to malaria-endemic areas are at risk of acquiring the disease.
Genetic Factors: Some individuals possess genetic traits that provide some protection against malaria.
Signs and Symptoms of Malaria
Malaria manifests through a variety of signs and symptoms, with feverbeing the most prominent and characteristic feature. The fever in malaria follows an intermittent pattern, coming and going repeatedly. A typical malaria attack can be categorized into three phases:
1. The Cold Stage:
Sudden onset of intense chills, often accompanied by shivering.
Sensation of coldness throughout the body.
2. The Hot Stage:
Intense heat and feverish feeling.
High fever, reaching 104°F (40°C) or higher.
Headache, often severe and localized to the frontal region.
Muscle pain, aches and stiffness, particularly in the back and limbs.
Nausea and vomiting, especially during febrile episodes.
3. The Sweating Stage:
Profuse sweating, often accompanied by a sense of relief from symptoms.
Other Symptoms Include:
A. Uncomplicated Malaria
i. In children under 5 years:
High fever: Detected by clinical thermometer, by touch, or reported by the caregiver.
Rigors: Shivering or trembling associated with the fever.
Loss of appetite: Reduced frequency of feeding, especially noticeable with breastfeeding.
Weakness and inactivity: Decreased energy levels and reduced movement.
Lethargy: Drowsiness and sluggishness.
Vomiting and diarrhea: These symptoms may accompany the fever.
ii. In older children and adults:
Fever: Recurrent fever, often accompanied by chills, sweating, and other symptoms.
Loss of appetite: Decreased desire for food.
Nausea and vomiting: Feeling sick to the stomach and throwing up.
Headache: Severe pain in the head, often localized to the frontal region.
Joint pains: Aching and stiffness in the joints.
Muscle aches: Soreness and pain in the muscles.
Weakness and lethargy: General fatigue and lack of energy.
B. Complicated/ Severe Malaria (Cerebral Malaria)
i. In children 5 years and below:
Signs of uncomplicated malaria plus any of the following:
Convulsions: Seizures within the last 2 days or currently present.
Inability to breastfeed or drink: Difficulty or refusal to feed.
Vomiting everything: Persistent vomiting, even after small amounts of food or fluids.
Extreme weakness (prostration): Inability to move or sit up.
Severe respiratory distress/ dyspnea: Difficulty breathing, rapid breathing, or labored breathing.
Severe anemia: Pale skin, fatigue, and shortness of breath due to low red blood cell count.
Severe dehydration: Dry mouth, sunken eyes, decreased urine output.
Hepatosplenomegaly: Enlargement of the liver and spleen.
Hemolytic jaundice: Yellowing of the skin and eyes due to destruction of red blood cells.
ii. In children 5 years and above (adults):
Signs of uncomplicated malaria plus any of the following:
Mental confusion and hallucinations: Disorientation, delirium, or seeing things that aren’t there.
Unconsciousness: Loss of consciousness.
Extreme weakness (unable to stand without support): Severe weakness and inability to stand without assistance.
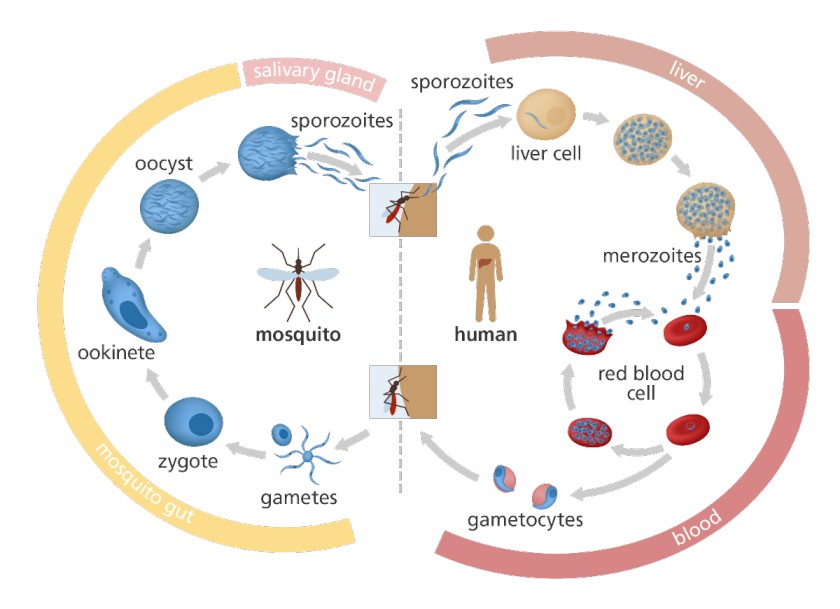
Illustration of the Malaria Parasite Life Cycle:
Malaria Parasite Life Cycle:
Infection begins when an infected female Anopheles mosquito bites a person, introducing Plasmodium sporozoitesinto the bloodstream.
The sporozoitesswiftly move into the human liver.
Over the next 7 to 10 days, the sporozoites multiply asexually in liver cells, causing no noticeable symptoms.
The parasites, now in the form of merozoites, are released from liver cells and travel through the heartto the lungs, where they settle within lung capillaries. The vesicles eventually disintegrate, releasing merozoitesinto the blood phase of their development.
In the bloodstream, the merozoites invade red blood cells (erythrocytes) and undergo further multiplication until the cells burst. They then invade more erythrocytes, repeating this cycle and causing fever each time they break free and infect new blood cells.
Some of the infected blood cells deviate from the asexual multiplication cycle and instead develop into sexual forms of the parasite known as gametocytes, which circulate in the bloodstream.
When a mosquito bites a human, it ingests these gametocytes, which further mature into sexually active gametes within the mosquito.
The fertilized female gametes transform into mobile ookinetesthat penetrate the mosquito’s midgut wall, forming oocystson its exterior surface.
Inside the oocyst, numerous active sporozoitesdevelop. Eventually, the oocyst bursts, releasing sporozoitesinto the mosquito’s body cavity, which then migrate to itssalivary glands.
The cycle of human infection begins anew when the mosquito bites another person.
Diagnosis of Malaria
Diagnosing malaria involves considering the patient’s clinical signs and symptoms, which can be challenging due to the similarity of malaria symptoms with other diseases, including yellow fever, typhoid fever, respiratory tract infections, meningitis, otitis media, tonsillitis, skin sepsis, and measles.
1. Clinical Evaluation:
Signs and Symptoms: Assess the patient’s clinical presentation, including fever, chills, sweating, headache, muscle pain, weakness, and any other relevant symptoms.
2. Laboratory Tests:
Microscopy:
Blood Smear Examination (Malaria Parasite Smear – MPS): This is the gold standard for malaria diagnosis. A blood sample is stained and examined under a microscope to identify the presence of malaria parasites within red blood cells. This test also helps to determine the specific species of Plasmodium responsible for the infection.
Rapid Diagnostic Tests (RDTs):
RDTs are antigen-based tests that detect specific malaria proteins in the blood. These tests are rapid and can be performed in resource-limited settings, but they may not be as sensitive as microscopy.
Quantitative Buffy Coat Test (QBCT):
This test estimates the number of red blood cells infected with malaria parasites by examining a centrifuged capillary tube. It is a more sensitive method for detecting low parasite densities, but it requires specialized equipment.
Complete Blood Count (CBC):
CBC evaluates various blood components, including red blood cells. Anemia (low red blood cell count) is commonly seen in malaria.
Hemoglobin Estimation:
Measures the amount of hemoglobin in the blood. Hemoglobin levels can be significantly reduced in malaria due to parasite-induced red blood cell destruction.
Liver Function Tests (LFTs):
These tests assess liver health, as the malaria parasites initially multiply in the liver.
Blood Chemistry Panel:
A blood chemistry panel evaluates electrolytes, kidney function, and liver enzymes, providing a comprehensive picture of the patient’s overall health status.
Polymerase Chain Reaction (PCR):
PCR is a highly sensitive molecular technique that can detect the genetic material of malaria parasites in the blood. This is particularly useful for diagnosing low-level parasitemia and differentiating between various Plasmodium species.
Serological Tests:
Serological tests detect antibodies produced by the body in response to malaria infection. They are not typically used for initial diagnosis but can be helpful for determining past exposure to malaria.
Management of Malaria
Treatment of malaria depends on the type of Plasmodium species, the severity of the disease, and patient-specific factors such as age, pregnancy status, and drug tolerance. Management is categorized into:
Management Of Uncomplicated Malaria
The recommended first-line medication for uncomplicated malaria is Artemether/Lumefantrine (Coartem).
In case Artemether/Lumefantrine is unavailable, the first-line alternative treatment is Atesunate + Amodiaquine.
The recommended second-line medication is Dihydroartemisinin + Piperaquine (Duocotecxin).
If not available, Quinine tables can be used.
For uncomplicated malaria, artemisinin-based combination therapies (ACTs) are the recommended first-line treatment. ACTs combine two drugs with different mechanisms of action, ensuring the rapid clearance of parasites and preventing drug resistance. Common ACTs include:
Administer the first dose under health supervision.
Fatty meals (including milk) enhance absorption.
If vomiting occurs within 20 minutes of swallowing the drug, the dose should be repeated.
Coartem is effective against blood schizonts and gametocytes, especially P. falciparum.
Not recommended for pregnant women in their first trimester or children weighing less than 5 kg. If ACTs are unavailable or contraindicated, alternatives like quinine or atovaquone-proguanil may be used.
Dosage Schedule for Coartem (Artemether + Lumefantrine):
Weight (kg)
Age
Day 1
Day 2
Day 3
5-14
4 months – 3 years
1 tab
1 tab
1 tab
15-24
3 – 7 years
2 tabs
2 tabs
2 tabs
25-34
7 – 12 years
3 tabs
3 tabs
3 tabs
>35
>12 years
4 tabs
4 tabs
4 tabs
Alternative First-Line Treatment:
Artesunate (50mg/tab) + Amodiaquine (153mg/tab)
Second-Line Treatment:
The recommended second-line medication is Dihydroartemisinin + Piperaquine (Duocotecxin). If not available,
Quinine Tablets (300mg/tab): Used if first-line treatment fails or is contraindicated (e.g., in pregnancy, children under 5 kg). Dosage depends on body weight.
Supportive Treatment
Antipyretics (Paracetamol): For fever reduction.
The dosage is ; Paracetamol – 10mg/kg body weight tds for 3 days.
AGE
NUMBER OF TABLETS/ MAX
2 months to 3 years
¼ to ¾
3 years to 7 years
1 to ½
7 years to 10 years
1 to 3
10 years to 15 years
1.5 to 4 ½
>15 years
2 to 6 tablets
Tepid sponging, fresh air, cold compress, fluids: To manage fever.
Nutrition: Light foods, plenty of fluids, and encouraging breastfeeding for infants.
Counseling And Health Education
Ensure the patient understands the cause of malaria and complies with the full course of treatment.
Educate on symptoms, the importance of completing treatment, and the need to consult a health worker if symptoms worsen or persist after two days.
Discuss prevention measures like sleeping under treated mosquito nets.
Treatment of Malaria
Treatment of Uncomplicated Malaria:
The recommended first-line medication for uncomplicated malaria is Artemether/Lumefantrine (Coartem).
In case Artemether/Lumefantrine is unavailable, the first-line alternative treatment is Atesunate + Amodiaquine.
The recommended second-line medication is Dihydroartemisinin + Piperaquine (Duocotecxin).
Treatment of Severe and Complicated Malaria:
Parenteral Artesunate is the recommended treatment for managing severe malaria in all patients.
In the absence of Artesunate, Parenteral Quinine or Artemether can be used as alternatives.
Treatment of Malaria in Pregnancy:
Uncomplicated malaria:
First trimester: Quinine tablets 60mg 8hourly for 7 days.(if Quinine not available, ACT may be used)
Second and third trimesters: First line, Dihydroartemisinin/Piperaquine 3 tablets(1080mg) once daily for 3 days. If no response, Quinine tablets.
Severe malaria in pregnancy should be treated with intravenous Artesunate 2.4mg/kg at 0, 12 and 24 hours, then once daily until mother can tolerate oral medication. Complete oral treatment with ACTs within 3 days.
Alternate first line: IM artemether 3.2 mg/kg loading dose then 1.6mg/Kg once daily until mother can tolerate oral medications. Complete ACTs within 3 days.
If artesunate or artemether not available, use Quinine 10mg/kg every 8 hours in Dextrose 5%.
Remember quinine is associated with an increased risk for hypoglycemia in late pregnancy.
Additional Treatment Measures:
Antipyretic to Reduce Body Temperature:
Paracetamol: 10mg/kg body weight every six hours in children, 1g 6-8 hourly in adults.
Tepid sponging or fanning can also be used to reduce fever.
Anticonvulsants:
Diazepam: 0.2mg/kg body weight intravenously or intramuscularly in adults.
Treat Detectable Causes of Convulsions:
For example, hypoglycemia can be managed with Dextrose administration.
Nursing Care:
Provide supportive care and symptomatic treatment, such as tepid sponging for fever.
Regularly observe temperature, pulse, respiration rate, and blood pressure. Record all observations.
Educate patients on personal protection, malaria prevention, and the importance of adhering to treatment.
Administer antiemetic medicine 30 minutes to 1 hour before antimalarial drugs if vomiting occurs.
Advise patients to rest for 1-2 hours after taking the medicine to avoid dizziness, vomiting, and hypotension.
Offer psychological support and comfort to patients.
Encourage a nourishing diet with plenty of oral fluids. In cases of difficulty in eating or drinking, consider passing a naso-gastric tube.
Monitor fluid intake and output and maintain a fluid balance chart.
Ensure proper patient and environmental hygiene.
Management of Severe Malaria (Cerebral Malaria)
This is a medical emergency requiring immediate and aggressive treatment.
A. At OPD/ Health Center Level:
i. Reception:
Welcome the patient and attendant: Establish a calm and supportive environment.
Resuscitative measures:
Establish an IV line: This is crucial for administering fluids and medications.
Infuse IV fluids: Use isotonic solutions like normal saline or Ringer’s lactate to raise blood pressure and combat dehydration.
Assess level of consciousness: Use the Glasgow Coma Scale (GCS) to assess the patient’s mental status.
ii. Urgent Treatment (First Aid Management):
Administer IM quinine: Inject 10mg/kg body weight of quinine intramuscularly (IM).
Control temperature: Use antipyretics like paracetamol (10mg/kg orally or per NGT).
Treat convulsions:
Rectal diazepam: Administer 5 to 10mg rectally for children.
IV diazepam: Use IV diazepam for adults.
Provide hydration:
Oral glucose: Administer via nasogastric tube (NGT) if the patient can swallow.
IV fluids: Infuse isotonic fluids to correct dehydration.
Counsel on transfer: Explain the urgency of transferring the patient to a higher level of care.
Write referral letter: Include the patient’s vital signs, medications administered, and the reason for referral.
NB: The patient’s well-being is paramount. Do everything possible to ensure safe and timely transport to a facility equipped to manage severe malaria.
B. At Health Center IV or Hospital Management:
i. Reception in Emergency Department/ Intensive Care Unit:
Assess briefly: Rapidly assess the patient’s condition, including vital signs, level of consciousness, and signs of respiratory distress.
Inform the doctor immediately: While simultaneously initiating resuscitative measures.
Resuscitation:
Airway management: Ensure a patent airway by clearing any obstruction.
Positioning: Place the patient in a comfortable position, typically supine with head slightly elevated.
IV line: Establish an IV line for fluid and medication administration.
Blood sample: Draw blood for:
Malaria parasite smear (B/S): For confirmation and species identification.
Hemoglobin (Hb) grouping and cross-matching: For blood transfusion if needed.
Hypertonic glucose: Administer a 50% dextrose bolus (0.5-1ml/kg in children, 30-50ml in adults) to treat potential hypoglycemia.
ii. Doctor’s Orders: Ensure the doctor’s orders are carried out promptly and effectively.
iii. Admission:
Admit to ICU/ Medical Ward: Select the appropriate unit based on the patient’s condition.
Equipment: Ensure the room is equipped with:
IV trays: For medication and fluid administration.
Oxygen apparatus: For oxygen therapy as needed.
Suction apparatus: For airway clearance.
Monitoring equipment: For continuous monitoring of vital signs.
Breathing equipment: Ventilator if needed.
Ventilation: Ensure the room is well-ventilated with fresh air.
Positioning: Maintain the patient in a comfortable and supportive position.
Oxygen therapy: Provide oxygen if the patient is dyspneic (having difficulty breathing) or anemic.
iv. Investigations:
Malaria parasite smear: Obtain a blood smear for confirmation and species identification.
Hemoglobin (Hb) grouping and cross-matching: Perform blood typing and cross-matching in preparation for potential transfusion.
Lumbar puncture (LP): Assist the physician in performing a lumbar puncture to rule out meningitis as a differential diagnosis.
v. Chemotherapy:
Intravenous quinine: Administer an intravenous infusion of quinine (10mg/kg body weight) in 5 to 10ml/kg of 5% glucose solution over 4 hours.
Avoid loading dose: Do not give a 20mg/kg loading dose as quinine can cause hypotension and hypoglycemia.
Maximum dose: Do not exceed the adult dose.
Dosage: Continue administering quinine at 10mg/kg every 8 hours until symptoms improve. After three doses, consider transitioning to oral quinine or a first-line artemisinin-based combination therapy (ACT) such as Coartem.
Anticonvulsants: Administer diazepam rectally (5 to 10mg PRN) or intramuscularly (IM 0.2mg/kg for children, 10mg for adults) for seizures.
Antipyretics- 10 mg/ kg orally or per NGT, 500 to 1000 mg (paracet); i.e 1 to 2 tabs. Adults tds. I.V fluids; oral fluids depending on the dehydration level.
Artemisinin-based combination therapy (ACT): After the initial quinine infusion, consider switching to an ACT like Coartem (artemether-lumefantrine) for continued treatment.
Dosage: Follow the specific dosage guidelines based on the patient’s weight and age.
Route: Administer orally, ensuring the patient swallows each tablet whole.
Duration: Continue for the recommended duration as per the treatment regimen.
Alternative ACTs: If Coartem is unavailable or not tolerated, other ACT options include:
Malarone: (atovaquone-proguanil)
Riamet: (artemether-piperaquine)
Asunapril: (artesunate-amodiaquine)
Other Anti-Malarials: Consider adding doxycycline (100mg twice daily for 7 days) if the patient has multidrug-resistant malaria or if the clinical response is poor.
Antifungal therapy: If there is suspicion of fungal infection (e.g., cryptococcal meningitis), initiate appropriate antifungal therapy, such as fluconazole.
Management of complications:
Cerebral edema:
Mannitol: Administer IV mannitol as a diuretic to reduce cerebral edema.
Corticosteroids: Consider using corticosteroids like dexamethasone to reduce inflammation.
Hypoglycemia: Monitor blood glucose levels regularly and administer IV dextrose if necessary.
Electrolyte imbalance: Monitor electrolyte levels and correct imbalances with appropriate solutions.
Hemoglobinuria: This may indicate severe hemolytic anemia. Consider blood transfusion if necessary.
vii. Supportive Care:
Oxygen therapy: Provide supplemental oxygen if the patient is hypoxic.
Fluids: Continue IV fluid administration to maintain adequate hydration.
Nutrition: Provide nutritional support via nasogastric tube (NGT) or parenteral nutrition if oral intake is inadequate.
Blood transfusion: Perform blood transfusion if necessary to manage anemia and maintain adequate blood volume.
Assess Anemia: Check for anemia and consider blood transfusion if necessary.
f. Acute Renal Failure:
Assess Cause: Determine if oliguria is due to shock or dehydration.
Frusemide: Administer frusemide as in pulmonary edema (above).
g. Convulsions:
Refer to: Management of Severe Malaria (see previous sections).
h. Coma:
Intensive Care: The patient requires admission to an intensive care unit (ICU).
Management:
IV Drip: Maintain an IV line for fluid and medication administration.
Urinary Catheter: Place a urinary catheter for monitoring urine output.
Nasogastric Tube (NGT): Place an NGT for nutritional support if necessary.
Positioning: Turn the patient every 2 hours to prevent pressure sores.
i. Hyperpyrexia:
Antipyretics: Administer antipyretics, such as paracetamol or ibuprofen.
j. Hemoglobinuria (Blackwater Fever):
Management:
Investigate and treat the cause.
Discontinue the suspected drug.
Steroids: Administer steroids (e.g., hydrocortisone, prednisolone, dexamethasone).
NURSING CARE
Feeding:
IV fluids: Administer IV fluids as needed.
Oral fluids: Encourage oral fluid intake.
Diet: Provide a soft, bland diet.
Other Nursing Care:
Hygiene: Maintain good personal hygiene.
Counseling: Provide psychosocial support (psychotherapy).
OTHER COMPLICATIONS
Hemolytic Jaundice: A complication of severe malaria.
Intrauterine Fetal Death (in Pregnancy): Can occur in pregnant women with severe malaria.
Hepatosplenomegaly: Enlargement of the liver and spleen.
Prevention and Control of Malaria
Implement Effective Treatment and Prophylaxis:
Early diagnosis and prompt treatment are essential to eliminate parasites from the human population. Timely treatment helps prevent the spread of malaria.
Vulnerable groups, such as pregnant women, should receive chemoprophylaxis (preventive medication). The following drugs are used for this purpose: Chloroquine, Doxycycline, Mefloquine, and Primaquine.
All pregnant women should be provided with Intermittent Preventive Treatment (IPT) to protect both the mother and the unborn child from malaria.
Reduce Human-Mosquito Contact:
Encourage the use of insecticide-treated nets (ITNs) while sleeping to create a physical barrier between individuals and malaria-carrying mosquitoes.
Implement indoor residual spraying of dwellings with insecticides or use knockdown sprays to control adult mosquitoes within households.
Advise individuals to wear clothing that covers the arms and legs, and to use mosquito repellent coils and creams when sitting outdoors at night to prevent mosquito bites.
Control Breeding Sites:
Eliminate stagnant water collection sites where mosquitoes breed, such as empty cans/containers, potholes, old car tires, and plastic bags. This can be achieved through proper disposal, draining, or covering with soil.
Use insecticides to treat stagnant water bodies to destroy mosquito larvae, or employ biological methods such as introducing larvae-eating fish to these water sources.
Provide Public Health Education:
Conduct public health education campaigns to raise awareness about malaria prevention measures, including the use of mosquito nets, personal protection measures, and the importance of seeking early diagnosis and treatment.
Educate communities about the significance of eliminating breeding sites and promoting good environmental hygiene to reduce mosquito populations.
Quick Quiz
Malaria Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Typhoid fever is an acute bacterial infection characterized by fever and is primarily spread through contaminated food and water.
Causes
Typhoid fever is caused by Salmonella typhi and Salmonella paratyphi A and B.
Enteric fever: A febrile inflammatory reaction due to the presence of bacteria in the intestines. Typhoid fever is a specific type of enteric fever caused by Salmonella Typhi.
Salmonellosis: A general term for infections caused by bacteria of the genus Salmonella. Typhoid fever is a specific type of salmonellosis caused by Salmonella Typhi.
Typhoid fever: A systemic infectious fever characterized by high fever, malaise, enteritis (inflammation of the intestines), rose-spot rash, and involvement of the lymphoid tissues (like the spleen). It is caused by the bacterium Salmonella Typhi.
Salmonella Typhi:
Classification: Salmonella Typhi belongs to the Enterobacteriaceae family, a group of bacteria commonly found in the intestines of mammals. They are flagellated (have hair-like structures for movement).
Characteristics:
Gram-negative: They stain pink when subjected to a Gram stain, a common diagnostic tool for bacteria.
Aerobic or facultatively aerobic: They can survive with or without oxygen.
Metabolism: They typically thrive at 37°C and utilize glucose and mannose for energy.
Antigens: Salmonella Typhi possess both cell wall antigens (O) and flagella antigens (H), which help them invade host cells.
Serological Testing: The serum (blood fluid) of infected patients can be used in agglutination tests, where the serum is mixed with specific antisera (antibodies) to detect the presence of O or H antigens.
Commensalism: Salmonella species are common commensals in the gastrointestinal tract (GIT) of poultry, domestic pets, birds, and humans. However, Salmonella Typhi is unique in that it only affects humans.
Predisposing Factors/Causes:
Inadequate hygiene: Poor handwashing after defecation/urination, especially in areas with inadequate sanitation, can lead to the spread of the bacteria.
Vectors: Flies, which can carry the bacteria on their bodies, can spread the infection.
Poor environmental hygiene: Lack of clean water, overcrowding, inadequate excreta disposal (lack of latrines) all contribute to the spread of typhoid fever.
Poor nutrition and poverty: Malnourished individuals and those living in poverty are more susceptible to infections, including typhoid fever.
Achlorhydria: Lack of stomach acid (HCl) can decrease the ability to kill the bacteria.
Schistosomiasis: This parasitic infection can compromise intestinal integrity, making it easier for bacteria to invade.
Homogenous sickle cell disease patients: Individuals with this genetic condition are more susceptible to infections.
Incidence:
Age group: Typhoid fever can affect individuals of any age, but the peak incidence is between 10 to 25 years. It is more common in women.
Dose of organisms:
A dose of 100,000 organisms can cause disease in 25% of individuals.
A dose of 1,000,000,000 organisms results in disease in 95% of cases.
Increasing the dose of bacteria generally leads to a shorter incubation period.
Gastric acidity (pH) plays a role in killing ingested bacteria, with low pH levels (more acidic) being more effective.
Incubation Period:
The incubation period for typhoid fever is usually 2 to 3 weeks.
Transmission
Typhoid fever is contracted by the ingestion of the bacteria in contaminated food or water.
Patients with acute illness can contaminate the surrounding water supply through stool, which contains a high concentration of the bacteria.
About 3-5% of patients become carriers of the bacteria after the acute illness. Some patients suffer a very mild illness that goes unrecognized, and these patients can become long-term carriers of the bacteria.
The bacteria multiply in the gallbladder, bile ducts, or liver and pass into the bowel.
The bacteria can survive for weeks in water or dried sewage.
The chronic carriers may have no symptoms and can be the source of new outbreaks of typhoid fever for many years.
Transmission Routes:
Contact with formites: Contact with objects contaminated with feces or urine from patients or carriers.
Flies: Flies can carry the bacteria and spread it through contact with food or surfaces.
Ingestion: The most common route of transmission is through ingestion of contaminated food or water.
Ano-oral transmission: Direct transmission from feces to mouth, especially prevalent in settings with high carrier rates, like prisons.
Signs and Symptoms of Typhoid Fever
Classically, the course of untreated typhoid fever is divided into four stages, each lasting approximately one week.
First week:
In the first week, there is a gradual rise in temperature (step-ladder fashion) accompanied by bradycardia, malaise, headache, generalized body aching, restlessness, and cough.
Epistaxis (nosebleeds) is observed in about a quarter of cases.
Abdominal pain may also be present.
Leukopenia, eosinopenia, and relative lymphocytosis are evident in blood tests.
The classic Widal test, used to detect antibodies against Salmonella, is negative in the first week, but blood culture reveals the presence of Salmonella typhi.
The payer patches of the distal end of the ileum are invaded by the bacillus and become inflamed, resulting in various manifestations such as slow pulse rate, severe persistent frontal headache, general malaise, anorexia, nausea, vomiting, intestinal upset (diarrhea and constipation), and depression of bone marrow.
Second week:
The payer patches form a slough (a layer of dead skin).
In the second week of the infection, the patient becomes severely ill with high fever, often reaching around 40°C (104°F), and bradycardia.
Delirium is common, characterized by a state of calmness or, at times, agitation.
Rose spots
Rose spots, which are pink spots, appear on the lower chest and abdomen in about one-third of patients.
The abdomen becomes distended and painful, especially in the right lower quadrant.
Diarrhea may occur, with stool appearing green and having a characteristic smell resembling pea soup. However, constipation can also be frequent.
The spleen and liver enlarge (hepatosplenomegaly) and become tender.
The Widal reaction shows strong positivity with anti-O and anti-H antibodies, while blood cultures may still be positive at this stage.
The tongue is coated with a brownish fur, and sordes indicate severe toxemia.
Dehydration becomes evident.
Third week:
In the third week of typhoid fever, several complications may arise:
The slough separates, leaving deep ulcers in the intestines.
Ulcers may erode blood vessels, leading to hemorrhage, or perforate the ileum, causing leakage of intestinal contents into the peritoneal cavity.
The patient becomes extremely ill and toxic.
Temperature remains very high and intermittent.
Pulse becomes feeble.
The patient lapses into a typhoid state, experiencing delirium and confusion.
Twitching of limbs may occur due to loss of calcium in the diarrhea state.
Carforragic picking may lead to clotting issues and blood-stained clothes.
Tough dries and flurried lips are observed due to severe dehydration from profuse diarrhea.
Signs of congestive cardiac failure (CCF) due to weakened myocardium may be present.
The patient may experience coma every eight hours.
Peritonitis, inflammation of the peritoneum, may occur.
By the end of the third week, the patient becomes emaciated, fever starts to subside, abdominal symptoms become more pronounced, and mental disturbances become prominent.
Fourth week:
The ulcers begin to heal through granulation.
At the beginning of the fourth week, the fever begins to decline, and the other symptoms gradually reduce as the patient’s temperature returns to normal.
Recovery is slow during this stage, and relapses are common.
If left untreated, typhoid fever can prove fatal in up to 25% of all cases.
To summarize;
Clinical Presentation:
Week 1 (Week of Onset):
Gradual onset: Symptoms typically develop gradually, but a sudden onset, especially with shivering and rigors (intense shaking chills), can occur in “paralytic typhoid.”
Progressive symptoms: Symptoms increase in severity over 3 to 4 days, often leading to bed rest.
Headache: A severe headache is common, accompanied by malaise, anorexia, limb pain, insomnia, and epistaxis (nosebleed).
Nausea and vomiting: The patient feels unwell, with nausea and vomiting.
Abdominal pain: Pain in the abdomen, often diffuse, with normal bowel movements or sounds initially. The abdomen may become distended with gas.
Constipation or diarrhea: Both constipation and diarrhea can occur.
Chest pain and cough: Chest pain and cough due to bronchitis are common.
Fever: The temperature rises steadily and remittently (fluctuates but does not return to normal) in a “step ladder” pattern, reaching 40-41°C within 24 to 48 hours. After a period of sustained fever, it starts to remit (decrease) at night and eventually resolves by lysis (gradual decrease).
Bradycardia: A slow pulse rate (70-90 bpm) is a classic sign of typhoid fever.
Splenomegaly and hepatomegaly: Enlargement of the spleen and liver.
Nerve deafness: Common in the first week.
Week 2 (Infective Week):
Ulceration and sloughing: Peyer’s patches ulcerate and slough off, and blood and necrotic tissue may be passed in the stool.
Sustained fever: The temperature remains high.
Increased pulse rate: The pulse rate increases while the volume decreases.
Abdominal distention and tenderness: The abdomen continues to distend and become tender, especially in the right iliac fossa (lower end of the ileum).
Offensive stool: The stool is foul-smelling and yellow, often described as having a “pea-soup” color.
Muscle aches: Muscle pain is prominent.
Rose spots: “Red-rose” spots appear on the chest and abdomen, usually starting around the 7th day and disappearing after 3 days.
Week 3 (Complications Week):
Increased toxaemia: Severe cases are marked by complications arising from increased toxaemia (toxins in the bloodstream), which spreads to various organs and systems.
Severe illness: The patient becomes very ill, confused, hallucinatory, and mentally apathetic, exhibiting carphologia (picking at the bedclothes).
Delirium: The patient develops moderate delirium.
Temperature falls by lysis: The temperature falls gradually.
Weak and rapid pulse: The pulse is weak and rapid, and the patient is anemic.
Dry mouth: The mouth is dry, the tongue turns brown, and halitosis (bad breath) is present.
Mouth ulcers: Ulcers develop on the gums and mouth.
Hot, dry, and jaundiced skin: The skin is hot, dry, and jaundiced.
Semiconsciousness: The patient may become semiconscious and incontinent of urine and stool.
Death: Death can occur in severe cases.
Week 4 (Recovery Week):
Convalescence: This is a period of gradual recovery.
Ulcer healing: The ulcers gradually granulate and heal between the 3rd and 5th week, usually without scar formation.
Improvement: The patient gradually improves, temperature returns to normal by lysis, and other symptoms subside.
Investigations for Typhoid Fever:
Stool Culture: Stool culture involves collecting a sample of the patient’s stool and incubating it under specific conditions to identify and isolate the causative bacteria, usually Salmonella typhi or Salmonella paratyphi. The presence of these bacteria in the stool confirms the diagnosis of typhoid fever.
Blood Culture: Blood sample is collected and cultured in a suitable medium to identify and isolate the bacteria causing typhoid fever. A blood culture is an effective method to confirm the diagnosis, especially in the early stages of the disease when stool cultures might be negative.
Widal Test: The Widal test is a serological test used to detect antibodies produced by the body in response to the infection by Salmonella typhi. The test measures the presence of specific antibodies, including anti-O and anti-H antibodies, in the patient’s blood. A positive Widal test suggests a recent or past infection with typhoid fever. However, it is important to note that the Widal test results should be interpreted cautiously, as false-positive results can occur due to cross-reactivity with other infections or previous vaccinations.
Additional Investigations (optional):
Polymerase Chain Reaction (PCR) Test: PCR is a molecular diagnostic test that can detect the genetic material (DNA or RNA) of the Salmonella bacteria directly from clinical samples, such as blood or stool. PCR is a highly sensitive and specific method, and it can provide rapid results, aiding in early detection and timely treatment of typhoid fever.
Typhoid Serology: Typhoid serology involves analyzing the patient’s blood for specific antibodies against Salmonella typhi. This test, similar to the Widal test, helps in confirming a recent or past infection, but it may have limitations in terms of sensitivity and specificity.
Complete Blood Count (CBC): A CBC is a routine blood test that provides information about the number and types of blood cells. In typhoid fever, the CBC may show leucopenia (low white blood cell count), eosinopenia (low eosinophil count), and relative lymphocytosis (increased lymphocyte percentage). These abnormalities can help in supporting the diagnosis of typhoid fever.
Liver Function Tests (LFTs): Liver function tests assess the health of the liver and its ability to function properly. In typhoid fever, liver involvement is common, and LFTs can reveal elevated liver enzymes and other liver-related abnormalities.
Urinalysis: Urinalysis may be performed to check for the presence of white blood cells or other indicators of kidney involvement, which can occur in severe cases of typhoid fever.
Complications of Typhoid Fever:
I. Gastrointestinal Complications: A. Perforation: The ulcerated areas in the intestines can lead to perforation, causing leakage of intestinal contents into the abdominal cavity. This can result in severe abdominal pain and peritonitis. B. Hemorrhage: The erosion of blood vessels by ulcers can cause gastrointestinal bleeding, leading to blood loss and anemia. C. Peritonitis: Perforation of the intestine can lead to peritonitis, an inflammation of the peritoneum (the lining of the abdominal cavity), causing severe abdominal pain and tenderness.
II. Gallbladder Complications: A. Cholecystitis: The infection can spread to the gallbladder, causing inflammation known as cholecystitis, which leads to abdominal pain, fever, and tenderness in the right upper abdomen.
III. Respiratory Complications: A. Pneumonia: In severe cases, typhoid fever can lead to pneumonia, a lung infection characterized by fever, cough, and difficulty breathing.
IV. Cardiovascular Complications: A. HeartFailure: Severe and untreated typhoid fever can put a strain on the heart, leading to congestive heart failure, a condition where the heart fails to pump blood effectively, resulting in fluid accumulation in the body.
V. Musculoskeletal Complications: A. Osteomyelitis: In rare cases, typhoid fever bacteria can spread to the bones, causing osteomyelitis, which is an infection of the bone and bone marrow.
VI. Neurological Complications: A. Encephalitis: Typhoid fever can lead to encephalitis, which is inflammation of the brain. This can cause symptoms such as headache, confusion, and altered mental state.
B. Meningitis: In some instances, the infection may also spread to the meninges, the protective membranes covering the brain and spinal cord, leading to meningitis.
C. Mental Confusion: During the advanced stages of the disease, mental confusion and delirium may occur due to the systemic effects of the infection on the central nervous system.
Management of Typhoid Fever
Hospital Admission:
In severe cases of typhoid fever, hospital admission is necessary to provide close monitoring and appropriate medical care.
Isolation or Barrier Nursing:
Patients with typhoid fever should be isolated or barrier nursed to prevent the spread of the infection to others.
Investigations:
Blood for Culture and Sensitivity (C/S) should be performed during the first week to identify the causative bacteria and determine its sensitivity to antibiotics.
Full Blood Sample (FBS) analysis will reveal low Hemoglobin (Hb) levels, low White Blood Cell (WBC) count, and an increased Erythrocyte Sedimentation Rate (ESR).
The Widal test can be done around 10/7 days after the onset of symptoms to detect antibodies against typhoid bacilli.
Blood Smear (B/S) examination should be conducted to rule out malaria.
Stool analysis and urinalysis are important to assess gastrointestinal and urinary involvement in typhoid fever.
Drug Therapy:
Antibiotic therapy is a cornerstone of typhoid fever management:
Ciprofloxacin at a dose of 500-750 mg twice daily for 10/7 (10 days).
Azithromycin at a dose of 10 mg/kg daily.
Cotrimoxazole at a dose of 960 mg twice daily for 3/7 (3 days) or as per a weight-based calculation for 10/7 (10 days).
Long-Term Carriers:
After signs have passed, stool tests should be conducted to check if Salmonella typhi bacilli are still present. Patients may become potential long-term carriers of the bacteria, requiring a 28-day course of antibiotics to eliminate the bacteria until they are free from it.
Fluid and Electrolyte Management:
Monitor intravenous (IV) fluid administration for rehydration.
Correct fluid and electrolyte imbalances with Normal Saline (N/S), Dextrose 5% (D5%) solutions, and oral fluids.
Nutrition:
Ensure adequate nutrition and provide a soft, easily digestible diet, unless the patient has abdominal complications or ileus.
Antipyretics:
Administer antipyretics like Paracetamol (PCM) to manage fever.
Hygiene and Infection Control:
Pay close attention to handwashing and limit close contact with individuals during the acute phase of the infection to prevent its spread.
Encourage proper waste disposal, covering of food, and proper food preparation to reduce contamination risks.
Encourage early screening and management to prevent the worsening of the disease.
Proper Water Treatment and Storage:
Educate patients on the proper treatment and storage of water to avoid waterborne transmission of the bacteria.
Regular Follow-Up and Monitoring:
Ensure regular follow-up and monitor for complications and clinical relapses.
Management of Delirium:
Encourage the use of Phenobarbital at a dose of 30-60 mg in case of delirium.
Treatment:
Antibiotic therapy:
Hospitalized patients: For hospitalized patients, treatment typically involves intravenous antibiotics, such as ceftriaxone or ciprofloxacin.
Hospitalized patients:
Ceftriaxone: 1-2 grams IV daily for 10-14 days.
Ciprofloxacin: 500-750mg IV twice daily for 10-14 days.
Non-hospitalized patients: For non-hospitalized patients with mild to moderate symptoms, oral antibiotics, such as ciprofloxacin or azithromycin, are often prescribed.
Non-hospitalized patients:
Ciprofloxacin: 500-750mg orally twice daily for 5-14 days.
Azithromycin: 500mg orally once daily for 3 days.
Supportive care: Provide supportive care, including:
Fluid replacement: Intravenous fluids or oral rehydration solutions are essential to prevent dehydration.
Pain management: Over-the-counter pain relievers can help manage pain and fever.
Nutritional support: Encourage adequate nutrition to support recovery.
Chronic Carriers:
Hospitalized patients: Hospitalized chronic carriers may require prolonged antibiotic therapy with medications like amoxicillin or ciprofloxacin.
Amoxicillin: 250mg orally three times daily for 4-6 weeks.
Ciprofloxacin: 500-750mg orally twice daily for 4-6 weeks.
Non-hospitalized patients: Non-hospitalized carriers may require ongoing monitoring and may be advised to avoid working in food-handling positions.
Immediate Nursing Care:
Rehydration: Provide intravenous fluids, nasogastric tube feeding, or oral rehydration solutions as needed to combat dehydration.
Temperature control: Implement tepid sponging and other measures to cool the patient’s temperature.
Mouth care: Provide oral hygiene to prevent mouth sores.
Nail care: Keep the patient’s nails trimmed and clean.
Perineal care: Keep the perineal area clean to prevent infection.
Personal protective equipment (PPE): Wear gloves, aprons, and goggles when handling anything from the patient to minimize exposure to bacteria.
Handwashing: Ensure frequent handwashing with soap and water and drying with clean towels.
Safe water and food: Use only treated or boiled water for drinking and cooking.
Disinfection: Dispose of wastes and excreta properly, disinfecting all contaminated items. Use disposable cups and plates whenever possible.
Non-disposable items: Disinfect non-disposable articles with concentrated disinfectants, replacing them regularly.
Linen treatment: Treat linens as infected material.
Terminal disinfection: Carry out terminal disinfection after the patient’s discharge.
Monitoring: Closely monitor the patient’s condition, particularly abdominal pain, diarrhea, constipation, and any signs of complications. Report any changes promptly.
Diet: Initially, provide a fluid diet high in calories, followed by a balanced, nutritious, soft diet (6-8 small meals).
Fluid and elimination: Monitor fluid intake and output, and assist with elimination as needed.
Psychological support: Offer emotional support to the patient.
Physiotherapy: Provide physiotherapy after the acute stage to help the patient regain strength and mobility.
Prevention:
Maintain cleanliness in the premises and ensure proper disposal of rubbish.
Keep hands clean and maintain trimmed fingernails.
Wash hands thoroughly with soap and water before eating or handling food and after using the toilet or changing diapers.
Drinking water should be free from microorganisms; it is preferable to boil water before consumption.
Avoid high-risk foods, such as raw or semi-cooked food.
During food preparation, wear clean, washable aprons, and caps.
Clean and wash food thoroughly, including scrubbing and rinsing fruits in clean water.
Store perishable food in the refrigerator, covering it properly.
Cook food thoroughly before consumption.
Consume food as soon as it is prepared.
If necessary, refrigerate cooked leftover food and consume it promptly. Reheat it thoroughly before consumption.
Exclude infected individuals and asymptomatic carriers from handling food and providing care to children.
Consider immunization, especially for those traveling to high-risk areas, where vaccines are available in oral and injectable forms.
Quick Quiz
Typhoid Fever Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Bacillary dysentery, also known as shigellosis, is an acute diarrheal disease of the intestines characterized by the passage of blood-stained mucoid stool.
It is a local bowel wall infection and does not spread systematically.
It is important not to confuse bacillary dysentery with diarrhea caused by other bacterial infections, as one of the distinguishing characteristics of bacillary dysentery is the presence of blood in the stool, resulting from the invasion of the pathogen into the mucosa.
Cause:
The causative agent of bacillary dysentery is the bacterium Shigella. There are four main species:
Shigella flexneri
Shigella sonnei
Shigella dysenteriae
Shigella boydii
Shigella dysenteriae is considered the most virulent. These bacteria are strictly pathogenic to humans with no animal reservoir.
Shigella are non-motile, gram-negative bacilli found in the gastrointestinal tract (GIT). They cause disease by invasion and destruction of the colonic mucosa using exotoxins.
Sources of Infection:
Symptomatic patients: Individuals actively experiencing symptoms of shigellosis.
Carriers: Individuals who harbor Shigella bacteria but show no symptoms.
Infective Dose:
The infective dose varies. As few as 10 to 100 viable Shigella organisms can cause dysentery, but about 10,000 are required for other species.
Incidence:
Shigellosis affects all age groups, particularly in areas with poor sanitation. It is more prevalent in tropical countries and less developed nations.
Incubation Period:
The incubation period for shigellosis ranges 1-3 days (can extend up to 7 days).Pathology:
All Shigella species have the ability to invade and destroy the epithelial cells of the large intestines. They produce exotoxins with enterotoxic, cytotoxic, and neurotoxic properties.
Enterotoxins: Produce a secretory effect on the intestine, similar to that caused by cholera toxin, leading to watery (secretory) diarrhea.
Cytotoxin: Binds to the cell surface and is transported inside cells, inhibiting protein synthesis and causing cell necrosis, which results in dysentery.
Neurotoxin: May be responsible for neurological complications in children but not adults.
Transmission Routes (Oro-fecal Route):
Person-to-person contact: Finger-to-mouth transmission is the most important means of transmission, especially among household members where hygienic habits are lacking. The infection is also common where there is ano-oral sexual contact.
Water-borne: Contamination of water supplies by sewage and excreta containing Shigella leads to outbreaks of shigellosis in communities.
Food-borne: Contaminated food and milk products are major sources of infection in hospitals and communities. Shigella can survive in various foods for up to 30 days under favorable conditions.
Flies: Flies can transmit the bacteria by settling on dysenteric stool and then contaminating food or utensils.
Predisposing Factors.
Shigellosis is a bacterial infection that occurs when a person ingests Shigella bacteria, usually through contaminated food or water. The bacteria then multiply in the intestines and invade the lining of the colon, causing inflammation and ulceration.
Defective sanitation: Poor refuse disposal contributes to the spread.
Bad hygienic practices: Poor excreta disposal, dirty hands, skin, and clothes, and inadequate cleaning of the anal orifice facilitate transmission.
Heavy environmental infestation with flies: Flies act as mechanical vectors.
Wet environment with stagnating water areas: These environments promote the survival of Shigella.
Signs and Symptoms:
The severity of symptoms varies depending on the amount of toxin produced, the infective dose, and the type of Shigella.
Mild Type (Watery Diarrhea): Onset is gradual, with tenesmus (a painful effort to defecate) that causes straining and painful defecation lasting for a few days after abdominal discomfort and the passage of watery stool.
Moderate Type: Abrupt onset with abdominal pain, nausea, and vomiting. The passage of blood-stained mucoid stool. Gripping and tenesmus may be severe, with dysuria. High fever and rigor. The face is pinched, and the look is anxious. The patient may become delirious and confused. Marked thirst.
Fulminating Type (Very Severe): Abrupt onset as described above. Watery diarrhea that later becomes bloody and mucoid. The patient may pass stool as frequently as 10 to 20 times in 24 hours (muco-purulent stools). The motions then decrease, and dysentery symptoms set in. Necrotic sloughs may be passed out. Severe abdominal cramps. Tenesmus. Profound prostration due to fluid loss. Toxaemia occurs from toxin absorption into the circulation. The cheeks are flushed, the expression is anxious, the pulse is rapid, the tongue is coated yellow or dry and furred and brown. Marked dehydration with oliguria, dry, shriveled skin, collapsed veins, low blood pressure. The urine contains albumin. The patient is restless and may die in uraemic coma. Perforation and peritonitis may occur, although rare, with abdominal distension and hiccups.
Other clinical features include;
Bloody diarrhea: Frequent watery diarrhea, often containing blood and mucus.
Abdominal cramps: Intense cramping pain in the abdomen. Flatulence
Fever: High fever, often accompanied by chills.
Tenesmus: A feeling of incomplete bowel emptying, with frequent straining and urgency to defecate.
Nausea and vomiting: Can occur, especially in severe cases.
Headache: General malaise and weakness.
Dehydration: Significant fluid loss can lead to dehydration, especially in young children and the elderly.
Electrolyte imbalance: Diarrhea can cause significant electrolyte loss, leading to imbalances that can be life-threatening.
Rectal prolapse: In severe cases, especially in children, the rectum can protrude from the anus.
Diagnosis/Investigations:
Stool culture: The most definitive diagnostic test involves culturing stool samples to identify the specific Shigella species present.
Stool analysis and appearance/rectal swab: Microscopic examination of stool or rectal swab for Shigella bacteria.
Microscopic examination: Stool examination under a microscope may reveal red blood cells, white blood cells, and bacteria.
Serological tests: Serological tests can detect antibodies to Shigella bacteria in the blood.
Differential Diagnosis:
Cholera: Similar symptoms, but cholera is usually more severe.
Acute diarrhea from food poisoning: Caused by different bacteria or toxins.
Amoebiasis: Caused by a protozoan parasite.
Ulcerative colitis: A chronic inflammatory disease of the colon.
Schistosomiasis from Schistosoma mansoni: Caused by a parasitic worm.
Carcinoma of the colon and rectum: Cancer of the colon or rectum.
Management:
Aims:
Prevent the spread of infection: Implement infection control measures.
Preserve and save the patient’s life: Prioritize life support.
Support patient recovery (nursing care): Provide supportive care.
Eliminate the offending bacteria (treatment): Administer antibiotics.
Management depends on the severity of the condition. Severe cases caused by Shigella dysenteriae are considered medical emergencies.
Severe Type of Dysentery (Medical Emergency):
First Aid Treatment:
The patient is received at the healthcare facility and assessed for airway, breathing, and circulation (ABCs).
Signs and symptoms of dehydration and anemia are assessed, and appropriate action is taken.
Brief history is taken, and observations are made. Pulse is checked. A doctor is called, and the patient is reviewed.
An intravenous (IV) line is established, and fluids such as glucose 50% (30 to 50 ml bolus), normal saline, or Ringer’s lactate (500 to 1000 ml) are connected to control blood pressure and correct electrolyte imbalance.
The patient and their attendant are reassured about hospital transfer and conditions.
The patient is referred to the hospital promptly.
Ward Management (Medical Emergency):
The patient is received and assessed with details from the initial healthcare facility report.
The patient is admitted in isolation, if possible. If not, high-level hygiene and infection control measures are put in place.
Disinfection of stool and vomitus with 1% sodium hypochlorite or other disinfectants.
Strict use of equipment and utensils only for that patient.
IV fluids are continued as per doctor’s orders.
Frequent monitoring of the patient (every 4 hours) for vital signs (including temperature, pulse, respiration, and blood pressure), signs and symptoms of dehydration, and signs and symptoms of anemia.
Immediate investigations are conducted:
Hemoglobin grouping and cross-matching for blood transfusions if needed.
Stool for analysis to identify the specific Shigella species.
Serum electrolytes to assess electrolyte balance.
Rectal swabs for bacterial culture.
Full blood count (FBC) and erythrocyte sedimentation rate (ESR).
Continuous Care in the Ward:
Patient’s personal and environmental hygiene: Similar to the management of cholera or typhoid fever.
Feeding: During the acute stages, a fluid diet is provided, followed by a soft, balanced, non-irritating, non-spiced, low-residue diet as the stool becomes more solid. Food hygiene is crucial.
Treatment:
Antibiotics: Nalidixic acid 1 mg every 6 hours for 5 days or ciprofloxacin 1 mg stat (immediately).
Pain killers: Paracetamol for children. Bactrim 24 mg/kg for children.
Vital signs and other assessments: Regular monitoring.
Nursing care: Provide supportive nursing care, including hygiene, comfort measures, and monitoring.
Urine and bowel care: Provide regular care and hygiene for the patient’s urinary and bowel functions.
Terminal disinfection: Thorough disinfection of the patient’s environment after discharge.
IMMEDIATE NURSING CARE:
Rehydration:
Intravenous fluids (e.g., Normal saline, Ringer’s lactate)
Oral rehydration solutions (e.g., ORS)
Hygiene:
Skin care: Keep the patient’s skin clean and dry.
Mouth care: Provide oral hygiene to prevent mouth sores.
Perineal care: Maintain meticulous perineal care to prevent skin breakdown.
Personal protective equipment (PPE):
Gloves, aprons, and goggles are worn when handling anything from the patient.
Handwashing: Frequent handwashing with soap and water and drying with clean towels.
Safe water and food: Use only treated or boiled water for drinking and cooking.
Disinfection: Dispose of wastes and excreta properly, disinfecting all contaminated items.
Linen treatment: Treat linens as infected material.
Terminal disinfection: Carry out terminal disinfection after the patient’s discharge.
Monitoring: Closely monitor the patient’s condition, particularly abdominal pain, diarrhea, constipation, and any signs of complications. Report any changes promptly.
Diet:
Initially, provide a clear liquid diet, avoiding dairy products.
Gradually transition to a bland diet, low in fiber, and avoiding spicy, fatty, and greasy foods.
Avoid contact: Avoid close contact with others until fully recovered.
Follow-up: Schedule a follow-up appointment with their healthcare provider.
summary;
Admission to a medical ward in isolation.
Strict personal hygiene (barrier nursing) to prevent infecting others.
Disinfection of the patient’s bed and other items used.
Proper disposal of fecal matter and vomit into a pit latrine.
Regular monitoring of temperature, pulse, respiration, blood pressure, hydration levels, and level of consciousness.
Providing reassurance and support to the patient and relatives.
Fluid intake maintenance using Oral Rehydration Solution (ORS) or intravenous fluids in severe cases.
Antibiotic treatment with drugs like nalidixic acid or ciprofloxacin.
Implementing a BRAT diet (bananas, rice, applesauce, toast) to aid in recovery.
Use of a nasogastric tube for feeding and medication administration if oral intake is not possible.
Medications for managing nausea and vomiting, such as metoclopramide (plasil).
Close monitoring of hydration levels and maintenance of a fluid balance chart.
Prevention:
Maintain cleanliness in premises and kitchen utensils.
Proper disposal of rubbish.
Practice proper hand hygiene before eating or handling food, and after using the toilet or changing diapers.
Boil or treat drinking water.
Avoid high-risk foods like shellfish, raw or semi-cooked food.
Use clean washable aprons and caps during food preparation.
Thoroughly clean and wash food items, including fruits, in clean water.
Store perishable food in a well-covered refrigerator.
Ensure thorough cooking of food before consumption.
Consume food promptly or refrigerate leftovers and reheat thoroughly before eating.
Exclude infected individuals and asymptomatic carriers from handling food or providing care to children.
Complications:
Perforation: A hole in the intestinal wall.
Hemorrhoids and rectal prolapse: Occur due to over-straining during defecation.
Hemolytic-uremic syndrome (HUS): A serious complication that can occur with Shigella dysenteriae infection, leading to kidney failure.
Stricture of the colon: Narrowing of the colon after healing.
Post-dysenteric colitis (irritable bowel syndrome): Persistent passage of stool after recovery, with colicky abdominal pain, which may clear after 6 months but may be permanent.
Dehydration: Fluid loss due to diarrhea.
Renal failure: Kidney dysfunction.
Shock (Hypovolemic): Low blood pressure due to fluid loss.
Severe intestinal hemorrhage: Bleeding in the intestines.
Comparison between Bacillary and Amoebic Dysentery:
Feature
Bacillary Dysentery
Amoebic Dysentery
Occurrence
Epidemic
Endemic
Severity
“Lying down disease”
“Walking disease”
Onset
Acute
Gradual
Fever
Common
Unless complicated
Tenderness
Whole abdomen, especially sigmoid part
Localized to sigmoid colon
Quantity of Stool
Scanty but very frequent, bright red, colorless, viscid mucus, jelly-like
Much mingled with blood and mucus, offensive, smelling of decomposing blood, copious
Tenesmus
Very severe
Present but mild
Stool Microscopy
Numerous RBCs, WBCs, and macrophages; few bacteria
Many RBCs in clumps; WBCs and macrophages are scanty; large number of mobile protozoa
Cause
Bacterial
Protozoal
Complications
Toxic arthritis and eye complications
Hepatic and other abscesses; skin perforations
Amoebic Dysentery (Amoebiasis)
Amoebic dysentery is a parasitic infection of the gastrointestinal system that is caused by the parasite Entamoeba histolytica.
The infection is most commonly acquired through oral-fecal contamination, which can occur by consuming contaminated food or water, or by coming into contact with contaminated feces and not washing your hands properly.
Symptoms of amoebic dysentery
Violent diarrhea, often with blood and/or mucus in the stools
Severe colitis
Frequent flatulence
Dehydration
Abdominal cramps and tenderness
Slight weight loss
Moderate anemia
Moderate fever
Mild fatigue
Unrelated symptoms such as liver abscess, lung involvement, amoeboma swelling, and anal ulceration
Diagnosis
The diagnosis of amoebic dysentery is usually made by examining a stool sample under a microscope to look for cysts or motile organisms. Ultrasound scans may also be performed.
Treatment
The treatment of amoebic dysentery involves several steps:
Correcting any dehydration
Initiating a 10-day course of the antimicrobial drug metronidazole (Flagyl) or tinidazole to eliminate the infection
Administering amoebicidal (lumenal) drugs such as diloxanide furoate, paromomycin, or iodoquinol to eradicate any remaining parasites
Isolating infected individuals to prevent further spread of the infection
Emphasizing personal hygiene practices
Prevention
To prevent the occurrence and transmission of amoebic dysentery, the following preventive measures should be followed:
Educate the public about proper handwashing before eating and appropriate fecal disposal practices.
Ensure the proper management of carriers of the infection.
Promote the use of clean drinking water and safe food handling practices.
Quick Quiz
Dysentery Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Cholera is an infection of the small intestine caused by the bacterium Vibrio cholerae.
Cholera is a serious, acute intestinal diarrheal disease characterized by a sudden onset of profuse watery stools, severe vomiting, rapid dehydration, acidosis, and circulatory collapse.
If left untreated, death can occur within a few hours after the onset of symptoms. Cholera is an internationally notifiable disease, meaning it must be reported to authorities, and it can spread to any part of the world.
The infection is characterized by profuse watery stools, vomiting, dehydration, and collapse.
Cause
Vibrio cholerae: This comma-shaped, gram-negative bacterium is responsible for cholera. It is aerobic or facultatively anaerobic, motile (using flagella), and thrives in alkaline environments (pH 8.0). It grows best at 30-40°C, but dies in acidic media or at temperatures below or above this range.
This bacterium is Gram stain negative and possesses a flagellum, a long projecting part that enables it to move, and pili, hair-like structures that it uses to attach to the intestinal tissue.
Mode of Spread
Fecal-Oral Route: The most common route of transmission is through contaminated water and food, which occurs when feces from an infected person contaminate water sources or food.
Ingestion of Contaminated Food: Ingesting food contaminated with infected water can lead to infection.
Direct Contact: Direct contact with an infected person, particularly without proper hygiene, can transmit the disease.
Carriers: Carriers of the bacteria, even if they are asymptomatic, can spread the disease to others.
Susceptibility: Several factors influence the susceptibility to cholera:
Ingestion of bacteria: In a normal, healthy adult, approximately 100 million bacteria must typically be ingested to cause cholera. This highlights the importance of a significant bacterial load for infection to occur.
Age: Children, particularly those between the ages of two and four, are more susceptible to cholera infection. This could be attributed to their underdeveloped immune systems and increased likelihood of exposure due to their behavior and hygiene practices.
Lowered immunity: Individuals with weakened immune systems, such as those with AIDS or malnourished children, are at higher risk of experiencing severe cases if they become infected with cholera. Their compromised immune function makes it more difficult for their bodies to fight off the infection effectively.
Pathology
Intestinal Colonization: Vibrio cholerae colonizes the small intestine and multiplies rapidly.
Enterotoxin Production: Vibrio cholerae produces cholera toxin, which doesn’t invade the intestinal mucosa or enter the bloodstream.
Fluid Secretion: The toxin disrupts the normal function of intestinal epithelial cells, causing them to secrete large amounts of fluids and electrolytes into the intestinal lumen. This results in profuse watery diarrhea.
Dehydration: The loss of fluids and electrolytes leads to severe dehydration. The body tries to compensate by drawing fluids from other areas, leading to:
Dry Skin and Mucous Membranes: The skin becomes dry, and the mucous membranes (including the eyes, mouth, and tongue) become dry.
Thickening of Blood: Blood becomes more viscous due to fluid loss.
Collapsed Vessels: Blood vessels collapse due to low blood volume.
Muscle Cramps: Severe muscle cramps result from electrolyte loss.
Lung Failure: The lungs become dry and may fail due to dehydration.
Organ Failure: Other organs can fail as a result of severe dehydration and electrolyte imbalance.
Pathophysiology of Cholera
Cholera is a gastrointestinal illness caused by the bacterium Vibrio cholerae. The bacteria produce a toxin that causes the body to lose water and electrolytes, leading to severe diarrhea.
How the Bacteria Enter the Body
MostVibrio cholerae bacteria are killed by the acidic environment of the stomach. However, a small number of bacteria can survive and travel to the small intestine. The bacteria attach to the intestinal wall and produce a toxin that causes the body to lose water and electrolytes.
The Toxin
The toxin produced by Vibrio cholerae is called cholera enterotoxin. The toxin binds to cells in the small intestine and activates an enzyme that causes the cells to pump water and electrolytes into the intestine. This results in the production of large amounts of watery diarrhea.
More Detailed Pathophysiology: Upon consumption, most Vibrio cholerae bacteria do not survive the acidic conditions of the human stomach. However, a small number of bacteria manage to survive. As they exit the stomach and reach the small intestine, they need to navigate through the thick mucus lining in order to reach the intestinal walls, where they can establish themselves and multiply. Vibrio cholerae bacteria possess flagella for mobility and pili to attach to the intestinal tissue.
Vibrio cholerae bacteria produce a toxin that is responsible for causing the most severe symptoms of cholera. This toxin, known as an enterotoxin, acts on human cells, prompting them to extract water and electrolytes from the body, primarily from the upper gastrointestinal tract. The extracted fluid and electrolytes are then pumped into the intestinal lumen, resulting in the excretion of diarrheal fluid.
Clinical Picture/Signs and Symptoms
The incubation period for cholera is usually 2-3 days. The first signs and symptoms of cholera are watery diarrhea and vomiting. The diarrhea can be so profuse that it can lead to dehydration and shock.
In a typical case of severe cholera, the disease progresses through three stages:
First Stage (Diarrheal Stage)
Onset: This stage lasts for 3 to 12 hours.
Profuse, Watery Diarrhea: The hallmark of cholera is the sudden onset of watery diarrhea, which can be profuse, ranging from several liters to 10 liters per day. The stool resembles rice water, a thin, milky white fluid that may contain flecks of mucus.
Vomiting: Vomiting may be frequent and can be severe, further contributing to dehydration.
Muscle Cramps: Muscle cramps, particularly in the legs and abdomen, are common due to electrolyte loss.
Mild Dehydration: Initially, dehydration is mild, but it can progress rapidly if not addressed promptly.
Second Stage (Collapse Stage)
Rapid Dehydration: This stage develops within 6 to 12 hours.
Increased Fluid Loss: Diarrhea and vomiting worsen, leading to rapid fluid loss and severe dehydration.
Thirst and Weakness: Intense thirst and general weakness become prominent.
Sunken Eyes and Dry Mucous Membranes: As dehydration progresses, sunken eyes and dry mucous membranes (mouth, tongue, eyes) are evident.
Skin Turgor and Skin Elasticity: Skin becomes dry and wrinkled, and skin turgor (the ability of the skin to return to its original shape after being pinched) is decreased.
Hypovolemia (Low Blood Volume): The decrease in blood volume leads to a rapid heartbeat, low blood pressure, and a weak pulse.
Hypotension (Low Blood Pressure): Hypotension can be profound, and blood pressure becomes difficult to measure.
Rapid Breathing: The body compensates for fluid loss by increasing the respiratory rate.
Electrolyte Imbalance: Loss of electrolytes (sodium, potassium, chloride, bicarbonate) can cause muscle cramps, fatigue, and confusion.
Acidosis (Increased Acid in Blood): Dehydration can lead to metabolic acidosis, which can cause rapid breathing, confusion, and lethargy.
Hypoxia: Lack of oxygen to the brain due to reduced blood flow can cause lethargy, confusion, and coma.
Third Stage (Shock Stage)
Life-Threatening: This stage is life-threatening, and immediate medical intervention is essential.
Circulatory Collapse: Severe dehydration leads to a collapse of the circulatory system, resulting in shock.
Rapid Heartbeat: The heart races in an attempt to maintain blood pressure.
Altered Mental Status: Confusion, lethargy, and coma are common.
Kidney Failure: Dehydration can lead to kidney failure.
Respiratory Failure: Severe dehydration can cause respiratory failure.
Diagnosis of Cholera
The diagnosis of cholera is based on the following:
History: The patient may have a history of travel to an area where cholera is common, or they may have been in contact with someone who has cholera.
Symptoms: The patient will typically have watery diarrhea and vomiting. The diarrhea may be so profuse that it can lead to dehydration and shock.
Physical examination: The doctor will examine the patient for signs of dehydration, such as dry skin, sunken eyes, and decreased urination.
Laboratory tests: The following laboratory tests may be performed to diagnose cholera:
Stool culture: This test is used to grow the bacteria in the laboratory.
Polymerase chain reaction (PCR): This test is used to detect the genetic material of the bacteria.
Rapid diagnostic test (RDT): This test is a rapid way to detect the bacteria.
Prevention of Cholera
Cholera is a serious disease that can be fatal, but it is preventable. The best way to prevent cholera is to follow proper sanitation practices.
Here are some specific steps you can take to prevent cholera:
Hand hygiene: Always wash hands with water and soap before preparing, serving, or consuming food. Additionally, it is important to wash hands with soap and water after using a latrine.
Safe drinking water: Boil all drinking water or treat it with chlorine. Store the treated water in a clean container to prevent recontamination.
Food safety: Consume food when it is still hot. If consuming raw foods such as fruits and vegetables, ensure they are properly washed, and when possible, peeled before eating.
Food storage: Cover all foods to prevent contamination by dust, house flies, and cockroaches.
Reporting and burial practices: In the unfortunate event of a cholera-related death, report it immediately to health authorities. Burial should take place promptly, and it is crucial to avoid serving food during this time.
Surveillance and reporting: Active surveillance and prompt reporting of suspected cases allow for the rapid containment of cholera epidemics.
Disinfection: Kill the germs by sprinkling germ-killing solutions, such as JIK, on stool or vomitus, as well as on any other materials used by the person suffering from cholera.
Water and sanitation improvement: Enhance water and sanitation infrastructure to reduce the transmission of infection, such as by improving access to clean water sources and implementing proper waste management systems.
Outbreak investigations: Conduct thorough investigations of diarrheal outbreaks to identify the source of contamination and implement appropriate control measures.
Cholera vaccination: Consider immunization with cholera vaccines in areas prone to outbreaks or for individuals at high risk of exposure.
Treatment of malnutrition: Address malnutrition, as individuals with weakened immune systems are more susceptible to severe cholera. Providing adequate nutrition can help improve their overall resilience.
Management and Treatment
Patient admission: The patient can be admitted to temporary hospitals, schools, or churches. Cholera beds with a central hole are used, allowing continuous stools to pass into a calibrated bucket containing a disinfectant.
Oral Rehydration Solution (ORS): ORS is the primary treatment for cholera. It is recommended for rehydrating patients and replenishing electrolytes lost through diarrhea. In cases of severe dehydration, intravenous Ringer’s lactate or normal saline, along with ORS, may be administered. The patient should be reassessed every one to two hours, and hydration should be continued. If there is no improvement in hydration, the intravenous drip rate may be increased. During the first 24 hours of treatment, the patient may require 200ml/kg or more of fluid. If hydration improves and the patient is able to drink, switching to ORS solution is recommended.
Nasogastric tube: In young children, a nasogastric tube can be used to administer fluids if necessary, ensuring adequate hydration.
Antibiotics: In certain cases, antibiotics may be prescribed. Doxycycline 300mg or ciprofloxacin as a single dose can be given, but they are contraindicated in pregnancy. For pregnant women, septrin can be used. In children, cotrimoxazole, doxycycline, ciprofloxacin, or erythromycin may be considered based on the specific circumstances.
Hypoglycemia management: If hypoglycemia is present, intravenous dextrose should be administered to correct low blood sugar levels.
Zinc supplementation: Zinc supplementation is effective in treating and preventing diarrhea, especially among children. It can be provided to aid in recovery.
Isolation and infection control: Patients should be isolated to prevent the spread of infection, as stools and vomit are highly infectious. Proper disposal of stools and vomit should be carried out, preferably into a pit latrine.
Equipment and instrument disinfection: Hospital equipment should be cleaned with a disinfectant such as JIK. Instruments can be cleaned with JIK or sterilized to prevent the transmission of the infection.
Fluid balance chart: A fluid balance chart should be instituted to monitor the patient’s hydration status closely.
Cholera Management:
Cholera is a medical emergency so prompt response should be initiated.
AIMS:
Immediate Reduction of Electrolyte and Fluid Loss: This is the primary goal, ensuring the patient’s survival.
Prevention of Infection Spread: Strict isolation measures are essential to prevent the spread of cholera within the healthcare setting and community.
Notification of Authorities: Promptly informing authorities about the outbreak is crucial for public health measures.
Elimination of Bacteria: Antibiotics are used to reduce the bacterial load and shorten the duration of illness.
Patient and Public Education: Raising awareness about cholera, its transmission, prevention, and proper management is essential for the community.
ACTIONS:
FIRST AID:
Reception: Properly protected healthcare personnel assess the patient’s airway, breathing, circulation (ABCs), signs and symptoms of dehydration (sunken eyes, dry mucous membranes, skin turgor), level of consciousness, and vital signs.
Immediate IV Line: Establish an intravenous line and begin fluid replacement with Ringers Lactate (R/L), Dextrose 5%, or Normal Saline, adjusting the rate according to the severity of dehydration.
Positioning and Oxygen: Place the patient in a comfortable position and provide oxygen therapy if necessary.
Hygiene: Ensure proper hygiene for the patient, including clean clothes, skin, and perineum.
History Taking: Gather detailed history, including the duration and severity of diarrhea and vomiting, level of consciousness, vital signs, and any relevant medical information.
Doctor’s Orders: Follow the doctor’s orders meticulously.
Treatment of Shock: Administer intravenous fluids as prescribed, usually starting with a rapid bolus of 100ml/kg over 30 minutes, followed by 70ml/kg over 2.5 hours. Reassess the patient’s response within 30 minutes to 1 hour. If there is no improvement, increase the rate of fluid administration.
Oxygen Therapy: Provide oxygen therapy as needed.
ADMISSION:
Isolation: Isolate the patient in a designated cholera bed with a central hole and bucket placed underneath for proper waste disposal.
Personal Protective Equipment: Healthcare personnel must wear appropriate personal protective equipment (PPE) when caring for the patient, including aprons, masks, isolation gowns, caps, gumboots, and disposable gloves. Explain the rationale for these measures to the patient.
District Health Authority: Inform the district health authority about the case for prompt public health action.
DRUGS:
Antibiotics:
Doxycycline: 300mg single dose OR
Ciprofloxacin: 1gm stat OR
Erythromycin: 62.5 to 250mg every 6 hours for 5 days OR
Ciprofloxacin: 20mg/kg single dose for children.
FREQUENT ASSESSMENT:
Vital Signs: Monitor vital signs every 15 minutes initially, then every 30 minutes, 1 hour, and 4 hours until discharge.
Dehydration Signs: Assess signs and symptoms of dehydration every 30 minutes, reclassify the severity, and adjust treatment accordingly.
Level of Consciousness: Observe the patient’s level of consciousness for signs of drowsiness, weakness, or confusion.
Fluid Output: Measure and record the volume, frequency, consistency, and characteristics of diarrhea and vomiting.
OTHER IMMEDIATE CARE:
Infection Control:
Disinfection: Disinfect all stool and vomitus with 1% sodium hypochlorite (JIK) before discarding.
Hygiene: Thoroughly clean and disinfect bedpans, buckets, urinals, and other contaminated items.
Patient Hygiene: Maintain patient hygiene by cleaning the skin, mouth, perineum, and providing padding as needed.
Linen Care: Soak contaminated linen in JIK for 2 to 6 hours, scrub thoroughly, place in labeled linen bags, and transport to the laundry for further disinfection.
Waste Disposal: Dispose of excreta and food remains after measurement and recordkeeping.
Utensil Care: Ensure the proper cleaning and disinfection of utensils.
Safe Water: Provide safe, boiled, and treated water for drinking and cooking.
Food Preparation: Ensure proper cooking of food and water treatment before consumption.
Environmental Hygiene: Thoroughly scrub sinks, equipment, and the patient’s room, labeling the room “Infectious, No Entry”.
Avoid Direct Contact: Minimize direct contact with patient’s waste.
DIET:
Parenteral Nutrition: Provide parenteral nutrition (IV or NG tube) in severe cases.
Fluid Diet: Start with a fluid diet (plenty of fluids) to rehydrate.
Light Diet: Gradually transition to a light, nourishing, well-balanced, non-irritating diet, considering the patient’s preferences and financial situation.
Normal Diet: Once the patient is stable, progress to a normal diet.
REHABILITATION/PHYSIOTHERAPY:
Passive ROM: Initiate passive range of motion exercises (ROM) while the patient is still in bed.
Active ROM: Encourage active sitting up in bed, moving to a chair, and walking around the room and outside for fresh air.
Reassurance: Continuously reassure the patient about their condition and their role in their recovery.
Health Teaching: Educate the patient about cholera:
Definition, causes, and mode of transmission
Importance of handwashing in infection control
Personal, community, and environmental sanitation or hygiene
Food and water hygiene and protection of water sources
Vector control using insecticide sprays
Reporting of new cases immediately
Mass screening, isolation, and treatment of suspected cases.
Limiting the use of equipment shared by infected individuals (showers, toilets, basins).
DISCHARGE:
Full Information: Discharge the patient with comprehensive information and follow-up dates.
Advice: Advise the patient on:
Adequate fluid intake
Good nutrition
Consumption of only safe food and water
Complications
Severe Dehydration and Vascular Collapse: This is the most serious complication of cholera, leading to circulatory shock and potentially death.
Electrolyte Imbalance and Acidosis: Severe fluid loss can disrupt electrolyte balance, leading to acidosis and potentially organ damage.
Shock: Dehydration can cause circulatory shock, a life-threatening condition.
Organ Failure: Dehydration and electrolyte imbalances can lead to heart, kidney, liver, and lung failure.
Hypoxia and Brain Malnutrition: Dehydration can cause hypoxia (lack of oxygen to the brain), leading to seizures, coma, and death.
Gangrene: Extreme fluid loss can lead to gangrene in the extremities due to reduced blood flow.
Hypostatic Pneumonia: Bedridden patients are at risk for hypostatic pneumonia due to reduced lung capacity.
Tetany: Electrolyte imbalances can lead to tetany, characterized by muscle spasms and seizures.
Acidosis: Dehydration and electrolyte imbalance can cause acidosis, a dangerous condition.
Abortion and Intrauterine Fetal Death: Severe diarrhea in pregnant women can increase intra-abdominal pressure, potentially leading to miscarriage or fetal death.
Prevention
Safe Water: Access to safe drinking water is crucial. Boiling water for 1 minute can kill Vibrio cholerae.
Handwashing: Frequent handwashing with soap and water, especially after using the toilet and before handling food, is essential.
Safe Food Handling: Proper food handling practices, such as cooking food thoroughly and storing it properly, can help prevent cholera.
Sanitation: Adequate sanitation facilities, such as latrines and sewage systems, are crucial for preventing the spread of cholera.
Vaccination: Oral cholera vaccines are available and provide partial protection against cholera infection. However, they are not always effective and require boosters for long-term protection.
Related Question
a) List 5 cardinal signs and symptoms of cholera.
b) Outline 10 specific nursing care in an outbreak of cholera.
Solutions
a) Five cardinal signs and symptoms of cholera include:
Watery diarrhea, sometimes in large volumes.
Nausea and vomiting.
Dehydration.
Rice-water stools.
Loss of skin elasticity.
b) Ten specific nursing care measures in an outbreak of cholera:
Wash hands with soap and running water frequently, especially after using the toilet and before handling food.
Advise people to drink only safe water, such as bottled water or water that has been boiled.
Encourage individuals to consume food that is fully cooked and hot, and to avoid street vendor food whenever possible.
Discourage the consumption of sushi, as well as raw or improperly cooked fish and seafood.
Monitor intake and output, taking note of the number, character, and amount of stools.
Promote the use of latrines or proper disposal of feces, emphasizing not to defecate in any body of water.
Ensure that any articles used are properly disinfected or sterilized before use.
Maintain strict asepsis during dressing changes, wound care, intravenous therapy, and catheter handling.
Practice hand hygiene by washing hands or using hand sanitizer before and after having contact with the patient.
Implement proper waste management procedures, particularly for human excreta.
Quick Quiz
Cholera Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Gastroenteritis (GE) is an acute medical condition characterized by the severe inflammation of the gastrointestinal tract. This inflammation involves both the stomach ("gastro-") and the small intestine ("entero-").
It typically results in a combination of acute diarrhea, vomiting, abdominal pain, and cramping. The severity of infectious gastroenteritis highly depends on the infected individual's immune system and its ability to resist the infection. A major clinical concern is the rapid loss of critical electrolytes (mainly sodium and potassium) as the individual vomits and experiences continuous diarrhea.
Causes of Gastroenteritis
Gastroenteritis can be triggered by a wide variety of pathogens, as well as non-infectious agents. The exact cause dictates the clinical presentation and management.
1. Viral Causes (Most Common)
Rotavirus: This is the single most common cause of severe gastroenteritis in infants and young children worldwide. It causes profuse, watery diarrhea.
Norovirus: The leading cause of viral gastroenteritis among adults. It is highly contagious and is responsible for greater than 90% of global gastroenteritis outbreaks (often in closed communities like cruise ships, hospitals, and schools).
Adenovirus & Astrovirus: Other common viral agents that predominantly cause GE in pediatric populations.
2. Bacterial Causes
Bacterial GE is often associated with foodborne illnesses (food poisoning) and poor sanitation.
Campylobacter jejuni: The primary cause of bacterial GE in the developed world. It is contracted by consuming raw or undercooked poultry meat, unpasteurized milk, or contaminated water.
Salmonella species: Contracted by ingesting the bacteria in contaminated food or water, and frequently linked to handling raw poultry and eggs.
Escherichia coli (E. coli): Various strains (like ETEC and EHEC) cause traveler's diarrhea and hemorrhagic colitis.
Shigella: Causes severe bacterial dysentery (bloody diarrhea with mucus).
Clostridium difficile (C. diff): An increasingly important cause of severe diarrhea, occurring more often in the elderly. It is highly associated with hospitalized patients and those with prolonged antibiotic use (which alters normal gut flora).
Staphylococcus aureus: Produces pre-formed toxins in food. Its infectious diarrhea can also occur in patients who have recently used broad-spectrum antibiotics.
3. Parasitic Causes
A number of protozoans can invade the intestines and cause prolonged GE, most commonly:
Giardia lamblia: Causes giardiasis, characterized by foul-smelling, fatty, and greasy stools.
Entamoeba histolytica: The causative agent of amoebic dysentery, which deeply invades the intestinal mucosa causing bloody stools.
Cryptosporidium: Causes severe, watery diarrhea, especially dangerous in immunocompromised patients (such as those with advanced HIV/AIDS).
4. Non-Infectious Causes
Medications: Use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) which irritate the gastric mucosa.
Dietary Intolerance: Certain foods such as lactose in individuals who lack the lactase enzyme (lactose intolerance).
Underlying Bowel Diseases: Conditions like Crohn’s disease, Ulcerative Colitis, and Celiac disease.
Heavy Metal Toxicity: Ingestion of toxins or heavy metals (e.g., arsenic, lead).
Transmission of Gastroenteritis
The transmission of GE germs occurs primarily through the fecal-oral route. This involves the accidental ingestion of feces or vomit particles from infected individuals. It is aggressively spread through the following means:
Consuming untreated, unboiled, or contaminated water from rivers, streams, lakes, ponds, or unprotected springs.
Eating cold, uncovered food that has been exposed to dust, mechanical vectors like house flies, or cockroaches.
Neglecting strict personal hygiene, specifically failing to wash hands with soap and water after using a latrine or before handling food.
Eating unwashed raw fruits and vegetables.
Serving food and drinks in dirty, unsterilized containers.
Storing safe drinking water in unclean containers, causing secondary contamination.
Improper and unhygienic disposal of human and animal feces in the environment.
The presence of open rubbish pits near homesteads that attract flies, rodents, and cockroaches.
Signs and Symptoms
The clinical presentation varies depending on the causative agent and the patient's age. However, the hallmark signs include:
Primary Symptoms: Acute, watery diarrhea often accompanied by sudden, forceful vomiting.
Stool Characteristics: Infected individuals may notice the presence of blood or mucus in their stools (indicative of dysentery caused by Shigella or E. histolytica).
Abdominal Discomfort: Severe, crampy abdominal pain is a common occurrence, which may temporarily ease immediately after passing stool.
Systemic Signs: Low-grade fever, persistent headache, lethargy, and generalized body aches (myalgia).
⚠️ Attention: Clinical Signs of Dehydration
Because fluid is lost rapidly, recognizing dehydration is critical to saving the patient's life. Symptoms include:
Mild to Moderate: Muscular cramps, sunken eyes, decreased urine output (oliguria), dry mouth and tongue, extreme weakness, and severe irritability. In infants, a sunken anterior fontanelle and absence of tears when crying.
Severe (Medical Emergency): Extreme fatigue, dizziness or lightheadedness, severe headache, confusion, rapid heart rate (tachycardia), deeply sunken eyes, skin pinching goes back very slowly (poor skin turgor), drastically reduced urine production (anuria), and eventually coma or death due to hypovolemic shock.
Diagnosis of Gastroenteritis
Clinical Assessment: GE is primarily diagnosed clinically, based on a comprehensive history of the person’s signs, symptoms, recent travel, and dietary intake.
Stool Analysis & Culture: Stool microscopy and cultures should be strictly performed, especially in patients presenting with blood or mucus in the stool, prolonged symptoms, or severe systemic illness. This helps isolate the exact bacteria or parasite.
Blood Tests: Serum electrolytes (to check for critical sodium and potassium imbalances) and a Complete Blood Count (CBC) may be requested in severe cases.
Clinical Management of Gastroenteritis
Gastroenteritis is usually an acute and self-limiting disease. The absolute primary goal of management is fluid and electrolyte replacement, not immediately stopping the diarrhea.
Oral Rehydration Therapy (ORT): The preferred and most effective treatment for mild to moderate dehydration. Oral Rehydration Salts (ORS) contain the perfect balance of water, glucose, and sodium to maximize intestinal absorption.
Alternative Fluids: Plain water, light soups, or rice water may be used temporarily if more specific and effective ORT preparations are completely unavailable or not palatable to the child.
Intravenous (IV) Fluid Delivery: Strongly required if there is a decreased level of consciousness (patient cannot drink), persistent vomiting, or if the dehydration is classified as severe. Ringer's Lactate or Normal Saline is commonly used.
Nasogastric (NG) Tube: Can be utilized in young, uncooperative children or those with severe nausea to administer life-saving ORS continuously.
Fluid Balance Monitoring: Institute a strict Fluid Balance Chart (Input and Output) to monitor the patient's hydration status.
Pharmacological & Nutritional Interventions
Zinc Supplementation: Highly effective and WHO-recommended in both treating and preventing diarrhea among young children. It reduces the duration and severity of the episode and prevents future episodes for up to 3 months.
Symptomatic Relief:Metoclopramide (antiemetic) may be helpful in controlling severe vomiting in some patients. Butylscopolamine (Buscopan) is highly useful in treating severe crampy abdominal pain (antispasmodic).
Dietary Adjustments: Breastfeeding must be continued on demand. Fermented milk products (such as yogurt containing probiotics) are highly beneficial in restoring normal gut flora.
Antibiotic Therapy: Antibiotics are not usually used for routine viral gastroenteritis. However, they are strictly recommended if symptoms are particularly severe (e.g., cholera, severe shigellosis), or if a susceptible bacterial cause is isolated or highly suspected.
If antibiotics are indicated, a macrolide (such as Azithromycin) is often preferred, or Ciprofloxacin for adults.
Metronidazole or Tinidazole is strictly used if the causative agent is a protozoa (e.g., Giardia or Amoeba).
Prevention and Control (Public Health Measures)
Preventing GE relies heavily on breaking the fecal-oral transmission cycle through strict hygiene and sanitation.
Strict Hand Hygiene: Always wash hands thoroughly with clean water and soap before preparing, serving, or eating food, and crucially, after using a latrine or changing a baby's diaper.
Water Safety: Boil all drinking water vigorously or treat it with approved chemical treatments (like chlorine/WaterGuard). Store safe water in clean, covered containers to prevent secondary contamination.
Food Safety: Consume food while it is still hot. Ensure that raw foods such as fruits and vegetables are properly washed with safe water and, whenever possible, peeled before eating. Cover all foods tightly to prevent contamination by dust, house flies, and cockroaches.
Infection Control & Disinfection: Isolate the severely infected patient to prevent cross-infection in wards. Kill germs by using strong germ-killing solutions like JIK (0.5% bleach solution) on stool, vomit, linens, and all other materials/surfaces used by the person suffering from diarrhea.
Environmental Sanitation: Improve community water sources and latrine coverage to permanently reduce the transmission of infection. Eliminate open rubbish pits.
Public Health Reporting: In the tragic event of a person’s death due to acute diarrhea (especially suspected Cholera), report it immediately to the local health authorities and conduct urgent epidemiological investigations of diarrheal outbreaks.
Address Co-morbidities: Aggressively treat underlying malnutrition, as malnourished children are significantly more likely to die from GE. Also, treat co-infections like typhoid and systemic dysentery.
Immunization: Strongly advocate for and ensure immunization with the Rotavirus vaccine (Rota vaccine) during the standard UNEPI schedule, which provides excellent, life-saving protection against rotavirus, the most deadly cause of gastroenteritis in infants.
💡 Quick Practice Check
Question: A 2-year-old child presents to the clinic with severe, watery diarrhea. The mother states the child has had no tears when crying and has not passed urine in 8 hours. What is the most critical immediate intervention?
Answer:Immediate Intravenous (IV) Fluid Resuscitation. The child is exhibiting signs of severe dehydration (anuria, lack of tears). While ORT is the standard for mild/moderate cases, severe dehydration requires immediate IV fluids (like Ringer's Lactate) to prevent hypovolemic shock and death, alongside Zinc supplementation.
References
World Health Organization (WHO) Guidelines on the Management of Acute Diarrhea and Use of Oral Rehydration Therapy.
Stanfield, B., & Versluys, M. (2004). Child Health: A Manual for Medical and Health Workers in Health Centres and Rural Hospitals (2nd ed.). English Press Limited, Nairobi.
Uganda Clinical Guidelines (UCG) on the Management of Gastroenteritis and Dysentery in Pediatric and Adult Populations.
Uganda National Expanded Programme on Immunization (UNEPI) Standards for Rotavirus Vaccination.
Quick Quiz
Gastroenteritis Quiz
Tropical Medicine - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.