
Leprosy (Hansen’s Disease) & National Management
1. Aetiology, Transmission, and Incubation
Cause of Leprosy (Aetiology)
Leprosy is caused by two specific types of bacteria:
- Mycobacterium leprae: The traditional, well-known bacillus responsible for the vast majority of leprosy cases globally.
- Mycobacterium lepromatosis: A relatively newly identified mycobacterium that was first isolated from a fatal case of diffuse lepromatous leprosy in 2008.
These bacteria are "acid-fast" and strongly prefer the cooler parts of the human body, which is why the disease heavily damages the skin, peripheral nerves near the body surface, the eyes, and the lining of the nose.
Transmission (Mode of Spread)
Leprosy is not highly contagious. It requires prolonged, close contact with an untreated infected person. The main routes of transmission include:
- Nasal Route (Droplet Infection): The bacteria are primarily spread through the air via infected nasal secretions when an untreated person sneezes or coughs.
- Transplacental: Transmission from an infected mother to her unborn baby across the placenta (rare but possible).
- Breast Feeding: Prolonged, close physical contact and transmission via breast milk.
- Genetic Predisposition: Modern science shows that over 95% of people are naturally immune to leprosy. However, certain individuals have a genetic weakness in their immune system that makes them highly susceptible to catching the disease when exposed.
Incubation Period
The incubation period refers to the time between when a person is first exposed to the bacteria and when the first signs of the disease actually appear on the body.
- The bacteria multiply exceptionally slowly.
- The standard incubation period usually lasts from 2 to 5 years.
- In severe cases, especially in Lepromatous leprosy, the bacteria can hide and grow for a much longer duration, taking anywhere from 8 to 12 years before obvious signs become apparent.
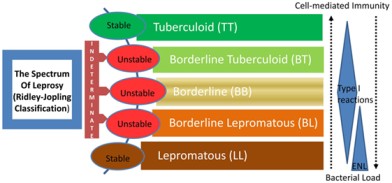
2. Types and Classification of Leprosy
Leprosy presents differently depending entirely on how strong the patient's cellular immune system is.
- 1. Lepromatous Leprosy (90% of cases):
This is the most common, severe, and highly infectious type. The patient has a very weak cellular immune response. Because the immune system cannot fight back, the bacteria multiply profusely all over the body. This leads to massive, widespread skin lesions and severe, permanent nerve damage. (In Uganda, 86% of new cases are this highly infectious 'multibacillary' type).
- 2. Tuberculoid Leprosy:
In this type, the patient has a much stronger immune response. The body fights the bacteria well, resulting in only a few, well-defined skin lesions. The affected skin patches may lose sensation, but the overall nerve damage is mild and much less severe compared to the lepromatous type.
- 3. Borderline Leprosy:
This type lies exactly in the middle between lepromatous and tuberculoid leprosy. The immune response is moderate. It displays mixed characteristics, showing a moderate number of skin lesions and moderate nerve involvement. If untreated, it can quickly downgrade into severe lepromatous leprosy.
- 4. Undeterminate (Dismorphoid) Leprosy:
This type is diagnosed in the very early stages of the disease when symptoms and the immune response are not yet well-defined. It is difficult to classify precisely. Over time, it will either heal on its own or develop into one of the major types listed above.
Clinical Differences Between the Major Types
| Cutaneous (Skin) Feature | Tuberculoid Leprosy | Borderline Leprosy | Lepromatous Leprosy |
|---|---|---|---|
| Number of Lesions | Very Few | Many | Many (Widespread) |
| Size of Lesion | Large | Both Large and Small | Small |
| Symmetry of Lesions | Asymmetrical (One side only) | Symmetrical (Both sides) | Symmetrical (Both sides) |
| Surface of Lesions | Rough and Scaly | Rough and Scaly | Smooth and Shiny |
| Edges of Lesions | Sharp and clear | Sharp | Vague and poorly defined |

3. Clinical Signs and Symptoms
Leprosy presents with a wide variety of signs that destroy both the patient's physical appearance and nervous system.
- Anaesthetic Skin Lesions: Patches of skin that completely lose their ability to feel sensation. The patient cannot detect pain, heat, cold, or light touch in these areas. Because they feel no pain, they frequently burn or cut themselves without noticing, leading to severe injuries.
- Thickened Peripheral Nerves: The bacteria invade the nerves, causing them to swell and become painfully thick. The midwife can easily feel these enlarged nerves as hard lumps under the skin (especially around the elbows and knees).
- Nasal Stuffiness: The bacteria attack the cool lining of the nose, causing chronic inflammation, swelling, and severe congestion.
- Saddled Nose: In advanced untreated cases, the bacteria completely eat away and destroy the cartilage inside the nose (nasal septum), causing the entire bridge of the nose to collapse flat.
- Loss of Eyebrows and Lashes: The disease destroys the hair follicles on the face, causing a complete loss of eyebrows and eyelashes (a condition medically known as Madarosis).
- Erythema Nodosum: Painful, red, raised nodules that erupt on the surface of the skin or deep under the skin's surface, usually during an immune reaction.
- Inflammatory Eye Changes: Leprosy attacks the facial nerves that control blinking. The eyes dry out, become inflamed, and develop ulcers, frequently leading to permanent vision impairment or blindness.
4. Investigations and Diagnosis
To officially diagnose leprosy and confirm the presence of the bacteria, healthcare professionals conduct several specific tests:
- Skin Snip / Slit-Skin Smear: A very small cut is made in the affected skin (usually the earlobe or lesion edge). The tissue fluid is smeared on a slide and stained using the modified Ziehl-Neelsen (ZN) method to visually identify the bacteria under a microscope.
- Polymerase Chain Reaction (PCR): An advanced molecular technique used to detect the exact genetic material (DNA) of the leprosy bacteria in skin samples. It is highly accurate and aids in very early diagnosis.
- Histamine Test: A drop of histamine is injected into the skin. A normal person will develop a bright red flare around the injection. In a leprosy patient, because the nerves are dead, there is no red flare. This test proves severe nerve damage.
- Lepromin Test: A substance derived from dead leprosy bacteria is injected under the skin. It measures how strongly the body's immune system reacts. It is not used to *diagnose* leprosy, but rather to determine the *type* of leprosy (e.g., Tuberculoid patients react strongly; Lepromatous patients have no reaction because their immunity is too weak).
🔍 National Strategy Focus: Early Case Finding
The Uganda Ministry of Health emphasizes aggressive Active Case Finding (ACF) to diagnose patients early. This involves house-to-house screening, school-based leprosy campaigns, and contact tracing. The goal is to catch the disease before it causes Grade 2 Disability (visible deformities), which is currently alarmingly high at 24% of new diagnoses.
5. Treatment and Management of Leprosy
Leprosy is 100% curable. Treatment relies heavily on Multi-Drug Therapy (MDT) to kill the bacteria completely and prevent them from developing drug resistance.
Primary MDT Drugs Used
| Leprosy Classification | Drug Combination Regimen |
|---|---|
| Tuberculoid Leprosy | Dapsone + Rifampicin (Usually taken for 6 months). |
| Borderline Leprosy | Dapsone (Often combined with Rifampicin depending on severity). |
| Lepromatous Leprosy | Dapsone + Rifampicin + Clofazimine (Taken for a minimum of 12 months, sometimes longer, to clear the massive bacterial load). |
Non-Leprosy Drugs Used in Management
- Steroids (e.g., Prednisolone): Used aggressively to calm down severe immune reactions and reduce inflammation around the nerves (neuritis), preventing permanent paralysis.
- Vitamin B Complex: Given routinely to nourish, protect, and promote the healing of damaged peripheral nerves.
Leprosy Prevention (National Guidelines)
- SDR-PEP (Single-Dose Rifampicin Post-Exposure Prophylaxis): Uganda's current strategy mandates tracing every person living in the same house as a leprosy patient. After checking them to ensure they don't already have the disease, they are given a single large dose of Rifampicin to kill any hiding bacteria and prevent them from ever falling sick.
6. Severe Complications of Leprosy
If diagnosis is delayed or treatment is not completed, the continuous nerve and skin damage leads to catastrophic, lifelong deformities. These include:
- Madarosis: The complete, permanent loss of eyebrows and eyelashes.
- Nasal Bridge Collapse: The "Saddle Nose" deformity resulting from the destruction of facial cartilage.
- Leonine Facies: The skin on the face becomes massively thickened, folded, and lumpy, giving the patient a frightening, lion-like facial appearance.
- Elongated Soft Ear Lobes: The earlobes swell with bacteria, becoming heavy, droopy, and permanently stretched.
- Ocular Complications: Paralysis of the eyelids means the eyes cannot close or blink. Dust and dryness cause severe corneal ulcers and eventual permanent blindness.
- Loss of Sensation: Total loss of the ability to feel heat, sharp pain, or light touch on the hands and feet.
- Multiple Ulcerations: Because the patient feels no pain, they repeatedly burn themselves on cooking fires or cut their feet on stones. These injuries become infected, forming deep, rotting ulcers.
- Nerve Enlargement: Hard, painful swelling of major peripheral nerves.
- Contractures & Shortening of Phalanges: The muscles in the hands become paralyzed and shrink. The fingers (especially the 4th and 5th fingers) curl into a rigid "claw hand." Over time, the bone tissue is reabsorbed by the body, making the fingers and toes incredibly short and stubby.
- Hammer Toes: Abnormal, rigid bending of the toe joints caused by muscle paralysis in the foot.
- Disuse Atrophy: Severe wasting and shrinking of muscles in different parts of the body because paralyzed limbs cannot be used.
- Orchitis: Severe, painful inflammation of the testicles as bacteria invade the reproductive organs.
- Sterility in Men: The secondary result of prolonged orchitis, permanently destroying the man's ability to produce sperm.
- Reactional States (Erythema Nodosum Leprosum): Ironically, when drug therapy successfully starts killing the bacteria, the immune system can suddenly overreact to the dead bacterial bodies. This causes massive fevers, nerve pain, and painful red skin lumps. It is an emergency requiring immediate steroids to save the nerves.
📝 Quick Clinical Review
Scenario: A patient is diagnosed with Lepromatous leprosy. Why are they at a much higher risk of developing deep foot ulcers compared to someone with Tuberculoid leprosy?
- Answer: Lepromatous leprosy involves massive, widespread bacterial growth due to a weak immune response. This results in severe, widespread destruction of the peripheral nerves. The patient completely loses pain sensation in their feet, meaning they will repeatedly step on sharp objects or walk on injured feet without knowing, leading to massive, deep, painless ulcers.
