
Safe Motherhood
Introduction to Safe Motherhood: Every single minute of every day, somewhere in the world (most often in a developing country), a woman dies from complications related to pregnancy or childbirth. That equates to a minimum of 515,000 women dying every year.
- 99% of maternal deaths occur in the developing world, making maternal mortality the health statistic with the largest disparity between developed and developing nations.
- For every woman who dies, 30 to 50 women suffer severe injury, infection, or disease.
- Pregnancy-related complications are among the leading causes of death and disability for women aged 15–49 in developing countries.
A woman's death is more than a personal tragedy. Children lose their primary caregiver, communities lose her unpaid and paid labor, and nations suffer an enormous cost to their economic and social development.
Definition & Origin of Safe Motherhood
Safe Motherhood Definition: This means ensuring that all women receive the exact care they need to be safe and healthy throughout pregnancy, childbirth, and the postpartum period. Safe motherhood ensures that no woman, fetus, or child should die or be harmed by pregnancy or birth.
It encompasses a series of initiatives, practices, protocols, and service delivery guidelines designed to ensure that women receive high-quality gynecological, family planning, prenatal, delivery, and postpartum care. It begins with the fundamental assurance of basic safety living as a girl and a woman in society.
- Origin: The Safe Motherhood Initiative (SMI) officially started in 1987 at an international conference held in Nairobi, Kenya.
- Initial Goal: The conference marked the beginning of a global initiative to reduce maternal mortality by 50% by the year 2000.
History and Evolution of Safe Motherhood (SMI)
The Safe Motherhood Initiative did not happen overnight; it evolved progressively from early global concerns into a highly targeted, worldwide movement.
- Early Efforts (1930s): According to AbouZahr (2003), the League of Nations noted and expressed deep concern regarding maternal mortality as early as the 1930s, especially concerning rapid industrialization and vertical medical programs.
- The UN Decade for Women (1976-1985): Efforts culminated during this decade, bringing women's overall health to the global stage.
- The Alma Ata Conference (1978): The WHO launched a comprehensive approach to health known as Primary Health Care (PHC), which strongly included maternal health.
- The Setback of the 1980s: The comprehensive PHC approach was short-lived. It was compromised by the introduction of Selective PHC (SPHC) in the 1980s. SPHC focused heavily on vertical programs (like family planning) while actual safety during pregnancy and childbirth was tragically neglected.
- The Turning Point (1985): Advances in statistical techniques unearthed grim insights. The WHO, supported by UNFPA, invested in community studies revealing that over 500,000 maternal deaths were occurring annually (99% in developing nations).
- Official Launch (1987): In February 1987, the WHO, UNFPA, and World Bank jointly sponsored the first international conference on Safe Motherhood in Nairobi, Kenya. Dr. Hafdan Mahler (then director of WHO) declared: "...something can, should—indeed must—be done, starting with the commitment of heads of states and governments."
3 Key Strategies of the 1987 Initiative (McGowan, 2017)
- Strengthening community-based health care.
- Building the capacity of referral-level facilities.
- Developing a rapid alarm and transport system to clearly link community and referral-level care.
Modern Integration: Safe motherhood has since been fully integrated into all global agendas. This includes the Millennium Development Goals (MDGs: 2000-2015) and the Sustainable Development Goals (SDGs: 2015-2030). Under SDG Goal 3 (target 3.1), the target is to reduce the global maternal mortality ratio to less than 70 per 100,000 live births by 2030.
⚠️ Points for Attention: The Dark Period of the 1980s
The shift from comprehensive PHC (1978) to Selective PHC (1980s) was a dark period for maternal survival. Global funding focused heavily on preventing pregnancies (family planning) rather than keeping women safe while they were actually delivering babies. The 1987 Nairobi conference corrected this fatal oversight.
Current Statistics & Scope of the Problem
According to the WHO (2017), the worldwide Maternal Mortality Rate (MMR) stands at 295 per 100,000 live births. Annually, approximately 585,000 to 600,000 women die of pregnancy-related complications (99% in developing countries, 1% in developed countries).
- Developed Countries: 11 per 100,000
- Low-Income Countries: 462 per 100,000
- Sub-Saharan Africa: 196 per 100,000
- Uganda: 336 (to 343 based on recent specific country stats) per 100,000
Annual Scope of the Global Problem
- 180-200 million pregnancies per year.
- 75 million unwanted pregnancies.
- 50 million induced abortions.
- 20 million unsafe abortions.
- 1 maternal death results in 30 maternal disabilities.
Developing vs. Developed Countries
| Developing Countries | Developed Countries |
|---|---|
| Weak health systems | Availability of robust data systems |
| Substandard quality of care | High professional expertise |
| Ineffective health services | Access to cost-effective technologies |
| Inadequate obstetric care | Enabling political conditions |
| Unregulated fertility | High awareness |
| High rates of infections | Strong commitment to act |
| Illiteracy & Ignorance | Ability to access affordable health services |
| Early marriage | - |
| Poverty & Malnutrition | - |
The State of Uganda
Uganda has the third fastest-growing population in the world. The systemic challenges and statistics are critical to understanding the local safe motherhood context:
- Total Fertility Rate: 6.9
- Maternal Mortality Ratio (MMR): 343 per 100,000
- Infant Mortality Rate (IMR): 97 per 1,000
- Child Mortality Rate: 147 per 1,000
- Unmet Need for Contraception: 28.4%
- Primary Education Completion: Only 34%
- Early Pregnancy: 70% of first pregnancies occur by age 19.
Systemic Challenges in Uganda
- While the Constitution guarantees women's rights, practical implementation takes time.
- Low levels of education for women and girls.
- Political and economic policies (e.g., World Bank and IMF policies) often do not favor African realities.
- Per capita spending on health is only $5, far less than the $40 recommended by the World Bank.
- Political will is often unfavorable to women's health (e.g., Sexual and Reproductive Health and Rights - SRHR services in school curriculums are still deemed unacceptable).
- The generally low status of women combined with extreme poverty.
Global Initiatives: ICPD and The Mother Baby Package
Following the 1987 Nairobi conference, global efforts continued to expand, spearheaded by the WHO, the United Nations Population Fund (UNFPA), the World Bank, and the United Nations Development Program (UNDP).
- The 1994 ICPD Conference (Cairo): During the Program of Action at the International Conference on Population and Development (ICPD) in 1994, a major global consensus was reached. It was agreed that meeting the reproductive health needs of women and men is a critical requirement for human and social development.
- Integration into Primary Health Care: The conference firmly affirmed that reproductive healthcare is not a separate, isolated issue; rather, it is an integral component of Primary Health Care (PHC) and must be provided within that context. The elements and components of reproductive health have a profound, direct impact on the course and outcome of pregnancy. Therefore, the health service requirements for addressing them are closely related.
- The WHO Mother Baby Package: It was during this 1994 conference that consensus was built to adopt a comprehensive strategy that addresses all aspects of reproductive health. This provided an opportunity to develop an integrated approach to safe delivery, which led directly to the creation of the WHO Mother Baby Package.
The "Making Pregnancy Safer" Strategy
After about 5 years of implementing the Mother Baby Package, the WHO and its global partners recognized the need to further improve maternal health and drastically reduce maternal mortality. This led to the introduction of the "Making Pregnancy Safer" strategy.
This strategy heavily emphasizes the importance of specific health sector interventions. If these six interventions are well implemented, they have the proven capacity to significantly reduce maternal mortality in any country:
- 1. Advocacy: Continuously raising awareness and speaking up for women's health at the community, national, and international political levels.
- 2. Partnerships: Building strong alliances between governments, health workers, donors, and non-governmental organizations to pool resources.
- 3. Improving National Capacity: Training more midwives, equipping hospitals, and strengthening the overall national healthcare system to handle obstetric emergencies.
- 4. Standard Setting and Tool Development: Creating clear, evidence-based clinical guidelines, protocols, and manuals for midwives and doctors to follow uniformly.
- 5. Research and Development: Continuously studying maternal health trends to find new, cost-effective technologies and medical solutions to save lives.
- 6. Monitoring and Evaluation: Keeping strict records and analyzing maternal data to see if the implemented programs are actually working and saving lives.
⚠️ Attention: Maternal Death as a Human Rights Issue
What is known worldwide about adverse maternal health is that a country’s overall economic wealth is not the only important determinant. According to national and international human rights treaties, safe motherhood is considered a fundamental human rights issue. Therefore, maternal death is a tragic reflection of a "social disadvantage," not merely a "health disadvantage."
Aims of Safe Motherhood
Note: Maternal and child health promotion is one of the key foundational commitments embedded in the WHO constitution.
The Safe Motherhood initiative is a global effort. It aims to improve women's health through deep social, community, and economic interventions. To achieve this, it relies on its partners: Government agencies, NGOs, and other local groups and individuals. The primary aims include:
- Hygienic and Accepted Medical Practices: To ensure that all deliveries are conducted safely, hygienically, and strictly according to accepted medical practices. This prevents iatrogenic complications (complications caused or exacerbated by poor care and dirty environments).
- Prompt Identification & Management: To identify obstetric complications promptly and manage them appropriately, either by treating the mother immediately at the facility or referring her to a higher level of care without delay.
- High Quality & Culturally Appropriate Care: Provision of high-quality care that respects the mother's culture. This ensures necessary follow-up and strong linkages with other critical services, including antenatal care, post-partum care, family planning, post-abortion care, and the treatment of STIs.
- Enhance Quality of Life: To deeply enhance the overall quality and safety of girls' and women's lives through the adaptation of a combination of health-related and non-health-related strategies (like education and economic empowerment).
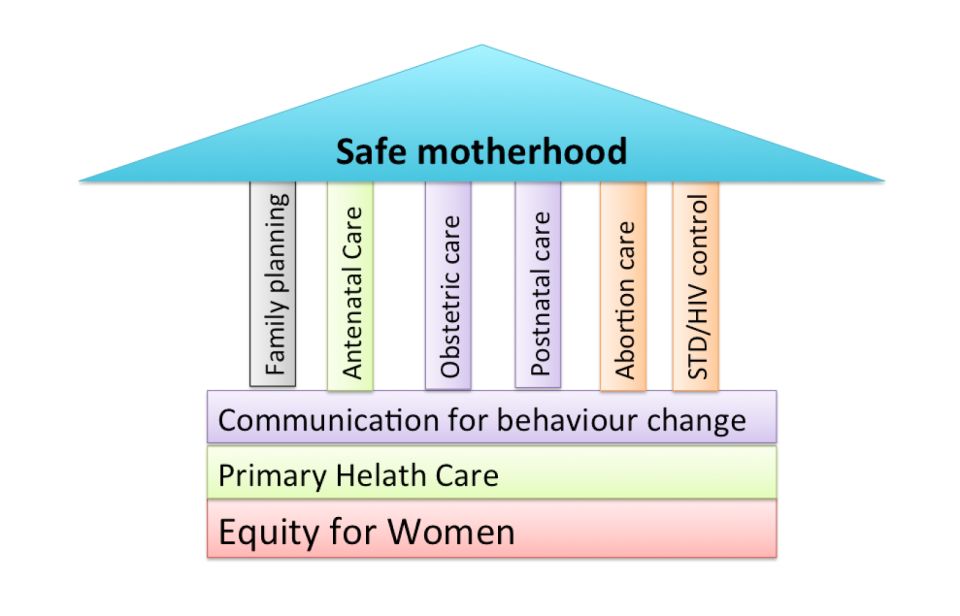
The Pillars of Safe Motherhood
The Safe Motherhood initiative is built upon a "house" of foundational structural pillars and key components:
- 1. Antenatal Care: Effective care is essential to detect preexisting conditions, prevent complications where possible, and ensure that serious conditions are treated appropriately and quickly.
- 2. Essential / Emergency Obstetric Care: Pregnancy is a period of potential risk for any woman (roughly 15% of normal pregnancies develop sudden complications). High-quality emergency care must be available to all women.
- Basic Emergency Obstetric Care (BEmOC): Includes basic first aid, IV antibiotics, oxytocic drugs, sedatives/anticonvulsants for eclampsia, manual removal of the placenta, and manual removal of retained products.
- Comprehensive Emergency Obstetric Care (CEmOC): Includes ALL BEmOC services, PLUS Surgery (Caesarean sections), Anaesthesia, and Blood transfusion capabilities.
- 3. Family Planning: Individuals and couples must have the information and services to plan the timing, number, and spacing of pregnancies to prevent unwanted pregnancies and unsafe abortions.
- 4. Postnatal Care: The critical first six weeks after childbirth. Most maternal and infant deaths occur during this time, yet it remains the most neglected period for the provision of quality care.
- 5. Abortion Care: Comprehensive abortion care includes safe abortion, post-abortion care, and family planning. (Note: Uganda currently only permits post-abortion care legally).
- 6. Equity for Women: Fairness of treatment according to respective needs. This includes equal treatment or equivalent treatment regarding rights, benefits, obligations, and opportunities.
- 7. STD/HIV Control: Prevent, detect, and treat STDs and HIV during pregnancy to prevent mother-to-child transmission (PMTCT) and protect maternal immunity.
- 8. Primary Health Care (PHC): Essential healthcare based on scientifically sound and socially acceptable methods, making universal healthcare accessible to all.
- 9. Communication for Behavior Change (SBCC/C4D): An interactive process to develop communication strategies promoting positive health behaviors appropriate to community settings.
❓ Applied Question: BEmOC vs CEmOC
Scenario: A rural health center is fully stocked with IV antibiotics, oxytocin for bleeding, magnesium sulfate for eclampsia, and the staff can manually remove a stuck placenta. However, they do not have an operating theater or a blood bank. Is this facility classified as BEmOC or CEmOC?
Answer: It is a BEmOC (Basic Emergency Obstetric Care) facility. To be classified as CEmOC (Comprehensive), a facility MUST have the capacity to perform surgery (like Caesarean sections) and administer blood transfusions.
Components and Requirements for Safe Motherhood
The 6 Core Components of Safe Motherhood
- Pre-conception care: Health and education before a woman even gets pregnant.
- Antenatal care: Close monitoring and education during the 9 months of pregnancy.
- Emergency obstetric care (EmOC): The ability to perform life-saving interventions (like C-sections or blood transfusions) when unexpected complications arise.
- Care of the newborn: Immediate resuscitation, warmth, and infection prevention for the baby.
- Postpartum care: Critical monitoring of the mother for bleeding and sepsis during the 6 weeks after delivery.
- Post-abortion care: Treating complications of miscarriage or unsafe abortions and providing family planning.
The 3-Way Strong Strategy (Requirements)
Achieving safe motherhood and permanently reducing maternal mortality strictly requires this 3-way strong strategy:
- Access to Contraception: All women must have easy access to modern contraception to avoid unintended, high-risk pregnancies.
- Skilled Attendance at Birth: All pregnant women must have access to a trained, skilled health worker (midwife or doctor) at the exact time of birth.
- Access to Emergency Care: All women who develop sudden complications must have timely access to quality emergency obstetric care.
The Roles of the Community in Safe Motherhood
Safe motherhood cannot be achieved by midwives alone within the hospital walls. The community must actively give support in several practical ways to make motherhood safer:
- Share the Workload: Family and community members must share household chores (like fetching water or farming) so that the pregnant mother can avoid heavy physical work that could trigger premature labour.
- Encourage Diet and Rest: Actively encourage the pregnant mother to eat a highly nutritious, balanced diet and to rest much more than usual, especially during the exhausting last three months of pregnancy.
- Ensure Medication Adherence: Encourage and remind mothers to take their iron/folic acid (non-pills) or other prescribed routine medications exactly as provided by the midwife.
- Assist with Childcare: Relatives or neighbors should help with looking after the older children so that the mother has the freedom and time to go for her antenatal care visits and to safely deliver in the hospital.
- Transport Readiness: The community leaders and families must establish transport readiness (e.g., saving money, identifying a vehicle or ambulance) well in advance for rapid emergency referral in case of obstetrical complications.
- Use of Maternity Waiting Areas: Strongly encourage high-risk mothers to travel early and use maternity waiting areas near the hospital, especially if they were advised to do so by the midwife during antenatal care.
- Safe Motherhood Groups: Create, inform, and heavily motivate community-based safe motherhood groups (like Village Health Teams) to continuously educate the village on maternal danger signs.
The Road Map to Safe Motherhood & Foundational Core
Safe motherhood is founded on freedom from discrimination, active participation, valuing the girl child, and ensuring access to care. The "Road Map" ensures maternal health is maintained throughout the life cycle:
- Childhood: Female children must have good nutrition for adequate growth and pelvic bone development (preventing future obstructed labour). They must be fully immunized against killer diseases.
- Adolescence: Girls should be educated about safe sexuality before experimentation to prevent early, unplanned pregnancies and STIs.
- Community & Family Support: A woman needs to be valued emotionally and physically. She should be relieved from heavy physical work during pregnancy. Communities must help organize referral transport systems.
- Antenatal to Puerperium: Mothers must be encouraged to attend ANC early. Traditional Birth Attendants (TBAs) must be educated to identify at-risk cases and refer them to hospitals instantly.
Global Initiatives & Conferences
- 1994 ICPD (Cairo): The International Conference on Population and Development established that reproductive health is an integral component of primary health care and a critical requirement for human development. This birthed the WHO Mother Baby Package.
- Making Pregnancy Safer Strategy: Five years after the Mother Baby Package, WHO introduced this strategy, emphasizing: Advocacy, Partnerships, Improving national capacity, Standard setting, R&D, and Monitoring/Evaluation.
- Social Disadvantage: Safe motherhood is a human rights issue. A maternal death is a reflection of a "social disadvantage, not merely a health disadvantage."
10 Priorities for Safe Motherhood (Action Messages)
During the 10th anniversary of the SMI, ten critical action messages were articulated summarizing the priorities needed to overcome economic, legal, social, and cultural barriers:
- Advance Safe Motherhood Through Human Rights: Preventing maternal death is social justice. Women have rights to life, health, privacy, liberty, and equality (free from discrimination and coercion).
- Empower Women, Ensure Choices: Maternal deaths are rooted in women's powerlessness and unequal access to employment, finances, and education. Legal reform and community mobilization are essential.
- A Vital Economic and Social Investment: National development plans must include safe motherhood. In developing countries, basic maternal and newborn care can cost as little as US$3 per person, per year.
- Delay Marriage and First Birth: Adolescent childbearing carries immense risks. Community education must encourage delaying marriage until women are physically, emotionally, and economically prepared.
- Every Pregnancy Faces Risks: Any woman can develop life-threatening complications. ANC programs should not waste resources solely on "risk-scoring," but must ensure emergency care is ready for all women.
- Ensure Skilled Attendance at Delivery: The single most critical intervention is ensuring a skilled health worker with midwifery skills is present at every birth, backed by emergency transport.
- Improve Access to Quality Reproductive Health Services: Health systems must address clinical, interpersonal, and logistical problems to overcome cultural customs that prevent women from seeking care.
- Prevent Unwanted Pregnancy & Address Unsafe Abortion: With 75 million unwanted pregnancies annually, unsafe abortion is the most neglected and easily preventable cause of maternal death. Client-centered family planning is vital.
- Measure Progress: Because maternal mortality is difficult to measure perfectly, alternative indicators must be used (e.g., recording the proportion of births attended by skilled personnel).
- The Power of Partnership: Reducing maternal mortality requires long-term commitment between governments, NGOs, donors, and community leaders.
⚠️ Points for Attention: Priority #5 (Risk Scoring)
Priority #5 marks a massive shift in public health. Historically, clinics tried to "score" women into low-risk and high-risk categories. We now know that every pregnancy faces risks, and emergencies (like postpartum hemorrhage) can happen to completely healthy women. Readiness for emergency care at delivery is far more important than risk-scoring.
Causes of Maternal Deaths
Direct Causes (Contribute to 75% of all maternal deaths):
- Severe bleeding (Hemorrhage): 31%
- High blood pressure during pregnancy (Eclampsia): 20%
- Infections (Sepsis): 1% to 15% globally depending on the region
- Complications from delivery (Obstructed labor): 7%
- Unsafe abortion
Indirect Causes (Contribute to ~25%):
- The Three Delays: (1) Delay in seeking care, (2) Delay in reaching care, (3) Delay in receiving care.
- Accessibility issues and extreme poverty.
- Harmful cultural practices.
Human Rights and Safe Motherhood
Preventing maternal death is fundamentally an issue of social justice and human rights.
- The Right to Life: Article 6 of the Political Covenant states every human has an inherent right to life. Maternity is a social function, not a disease. Emergency obstetric care must be accessible to preserve life.
- Rights Relating to Pregnancy and Childbirth: Women are entitled to special protection, paid maternity leave, and must not suffer employment discrimination.
- Rights Relating to Discrimination: Neglecting maternity care constitutes sex discrimination. For example, requiring a husband's spousal consent for maternal care (which men do not need for their own care) is highly discriminatory.
- Fertility by Choice: Article 16 of the Women's Convention grants women the right to decide freely on the number and spacing of children. Denying family planning coerces women into motherhood.
- Rights to Health (Sexual & Reproductive): Entitles women (including HIV-positive women needing PMTCT) to the highest attainable standard of health via functioning, accessible facilities.
- Rights to Privacy, Liberty, and Security: Women must be empowered to decide for themselves when to seek health care without the cruel/degrading requirement of spousal permission.
- Rights to Education and Information: Crucial for raising awareness of safe motherhood and identifying danger signs.
⚠️ Points for Attention: Human Rights Violation
If a woman dies because society deemed her unworthy of a $5 transport fare to a clinic, or because her husband refused to give "permission" for her to leave the house, her death is a severe human rights violation, not just a medical failure.
Enablers and Preventing Factors of Safe Motherhood
| Enablers of Safe Motherhood | Preventing Factors (Barriers) |
|---|---|
| Antenatal care provided directly in the village. | No trained midwives available to the community. |
| A good, fast system of emergency referral. | Untrained TBAs handling complicated deliveries. |
| Safe motherhood committees driving community ownership. | No working relationships with community leaders. |
| Maternity waiting homes for women living far away. | No transport available for emergencies. |
| Male involvement and deployment of Village Health Teams (VHTs). | Severe poverty and poor road infrastructure (especially in rain). |
| Mobile health (mHealth) reminders and elimination of user fees. | Drug/blood stock-outs and ingrained cultural myths against medicine. |
📋 Assignment & Framework: The 3-Delay Model
Prompt: Discuss the 3-delay model as it relates to access to maternal and newborn care by women and girls.
Concept Breakdown (The 3 Delays):
- Delay 1 (Deciding to seek care): Driven by a lack of knowledge of danger signs, cultural beliefs, reliance on traditional healers, or women lacking the financial/decision-making autonomy to leave the house without permission.
- Delay 2 (Reaching the facility): Driven by vast geographical distances, poor road conditions, lack of ambulances/transportation, or total inability to pay for transport.
- Delay 3 (Receiving quality care): Driven by understaffed clinics, poorly trained workers, lack of essential equipment/drugs, lack of a blood bank, or poor staff attitude resulting in lethal neglect.
Test yourself: If a woman arrives at a clinic in active labor but bleeds to death because the clinic has no IV oxytocin or blood transfusions available, which Delay caused her death? Answer: Delay 3.