
Labour (Normal Labour)
Labour is the natural process by which the fetus, placenta, and membranes (the products of conception) are expelled from the mother's womb through the birth canal after 28 weeks of pregnancy.
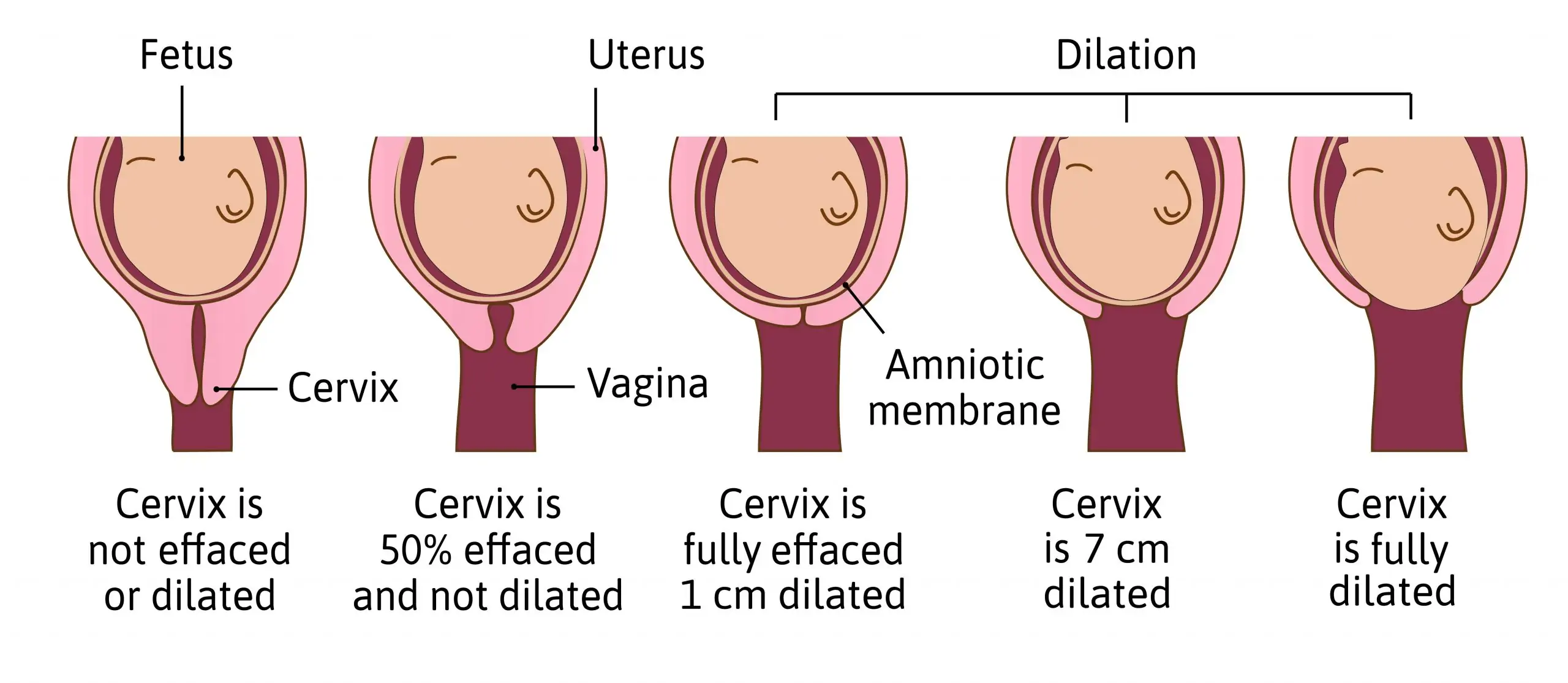
In medical terms, labour is defined as the rhythmic contraction and relaxation of the uterine muscles. This causes the cervix to progressively thin out (effacement) and open up (dilatation), eventually pushing the baby out into the world.
What is Normal Labour?
For a midwife to classify a mother's labour as Normal Labour, it must carefully meet all the following conditions:
- Occurs at term: The pregnancy must be between 37 and 42 weeks.
- Spontaneous in onset: Labour starts on its own naturally, without the use of drugs or artificial methods to induce it.
- Fetus presenting by vertex: The baby is coming out head-first (the head is pointing downwards).
- Completed within normal time: The whole process should be completed within 12 to 18 hours.
- No complications arise: Everything goes smoothly without emergencies.
- No injury: Both the mother and the fetus suffer no harm or injury during the process.
- No artificial assistance is given: The baby is born naturally without the need for vacuums, forceps, or surgery.
The Three P’s of Normal Labour
For normal labour to be successful, three important factors must work perfectly together. We call these the "Three P's":
- Powers: This refers to the strength of the uterine contractions. Strong, regular contractions are needed to push the baby down.
- Passage: This refers to the mother's pelvis, including its size and shape, as well as the soft tissues of the birth canal. It must be wide enough for the baby to pass through.
- Passenger: This refers to the fetus itself (its size, position, and presentation) as well as the bag of fore-waters (the amniotic sac).
🧠 Easy Memory Aid for the 3 P's
Imagine a train journey: The Powers are the engine pushing, the Passage is the railway track, and the Passenger is the baby taking the ride!
Types of Labour (True vs. False)
It is very common for mothers to feel pains and think they are in labour when they are actually not. Midwives must know how to tell the difference between True Labour and False Labour.
| Feature | True Labour | False Labour |
|---|---|---|
| Contractions | Regular rhythm. Start mild but increase in severity (strength) and frequency. | Irregular. No clear rhythm. Pain is continuous without rhythm. |
| Cervical Dilatation | Causes the cervix to progressively open (dilate). | No cervical dilatation happens at all. |
| Pain Location | Starts in the back and radiates to the front of the abdomen. Associated with stomach hardening. | Pain remains stationary in the lower abdomen. No associated hardening of the abdomen. |
| Effect of Movement | Pain gets stronger when walking or moving around. | Pain appears stronger when in bed and weaker when the mother is up and walking. |
| Show (Mucus plug) | Present (Bloody show is seen). | No show. |
| Effect of Enema/Rest | Pain continues and gets stronger. | Pain often reduces or stops after an enema, resting, or drinking water. |
Signs of Impending Labour (Pre-Labour)
These are changes that happen in the mother's body during the last few weeks of pregnancy to prepare for birth. This period is termed as pre-labour.
- Lightening: About 2 to 3 weeks before labour starts, the lower part of the uterus expands. This allows the baby's head to sink lower into the pelvis. The pelvic bone (symphysis pubis) widens, and the pelvic floor relaxes to let the uterus descend further. Because the baby drops, the mother feels lighter and can breathe easier.
- Cervical changes: As labour gets closer, the cervix becomes "ripe." It changes from being hard like a nose to being soft like a lower lip. It also starts to thin out (effacement) and open very slightly.
- False labour: As explained above, the mother may experience painful uterine contractions that do not open the cervix. These are exaggerated Braxton Hicks contractions (practice contractions) which have been occurring painlessly since 6 weeks. False labour can happen on and off for days, or even 3 to 4 weeks before true labour begins.
- Premature Rupture of Membranes (PROM): Normally, the water breaks (membranes rupture) at the end of the 1st stage of labour. But if the water breaks before labour starts, it is called PROM. This happens in about 12% of women. For 90% of these women, true labour will start on its own within 24 hours.
- Bloody show: Throughout pregnancy, a thick mucus plug sits in the cervix to block infections. As the cervix softens and slightly opens, this mucus plug falls out, mixed with a little blood. This is called the bloody show.
- Energy spurt: Many women experience a sudden burst of energy about 24 to 48 hours before labour. After feeling tired for weeks, they suddenly wake up full of energy and vigor (often cleaning the house, known as the "nesting instinct").
- G.I.T upset: Some mothers experience unexplained diarrhea, nausea, vomiting, and indigestion just before labour begins. If there is no illness causing this, it is considered a sign that the body is preparing for labour.
Signs of Labour
The signs that labour has actually begun are divided into two main categories: Premonitory signs and Actual signs.
1. Premonitory Signs (Warning Signs)
- Lightening: As discussed, it occurs 2-3 weeks before labour. The head sinks to engage in the pelvis, taking pressure off the mother's lungs, giving her relief.
- Frequency of micturition (Urination): As the baby drops deep into the pelvis, it limits the space for the bladder. The mother will need to pass urine very often.
- Effacement of the cervix: This is the "taking up" of the cervix. The cervix is pulled up and smoothly merges into the lower part of the uterus, becoming very thin.
- Braxton Hick’s contractions: These practice contractions become stronger and make the mother anxious. She will feel backache and pain while walking because her pelvic joints are relaxing.
2. Actual Signs (True Proof of Labour)
- Regular uterine contractions: The mother feels painful, rhythmic contractions that start out mild but quickly increase in severity (pain) and frequency (how often they come).
- Dilatation of the cervix: The external opening of the cervix (the OS) enlarges from a tiny circle into an opening wide enough to allow the baby to pass through (up to 10cm).
- Show: The bloody, mucus-like discharge comes out. As the cervix opens, tiny blood vessels (capillaries) tear, mixing blood with the mucus plug.
- Rupture of membranes: The breaking of the water. However, midwives do not rely on this as a sure sign of early labour, because the water can break very late in the 1st stage or even spontaneously right as the baby is born.
Causes of the Onset of Labour
The exact trigger that starts labour remains a medical mystery, but it is highly believed to be a combination of hormonal factors and mechanical factors.
Hormonal Factors (Theories)
- Oxytocin stimulation theory: As pregnancy reaches its end, the uterus becomes highly sensitive to the hormone oxytocin. Oxytocin causes strong muscle contractions.
- Progesterone withdrawal theory: Progesterone is the hormone that relaxes the uterus and keeps the pregnancy safe. Near the end of pregnancy, progesterone levels drop. This removes the relaxing effect, allowing the uterus to start contracting.
- Oestrogen stimulation theory: Oestrogen makes the uterine muscles irritable and ready to contract. A rise in oestrogen forces the lining of the womb (decidua) to release prostaglandins. Both prostaglandins and oxytocin work together to make the uterus contract.
- Fetal cortisol theory: The baby's own body produces cortisol (a stress hormone) when it is ready to be born. This fetal cortisol affects the mother's oestrogen levels, triggering labour.
- Prostaglandin stimulation theory: Prostaglandins directly stimulate the smooth muscles of the uterus to contract violently, pushing the baby down.
Mechanical Factors
- Over-stretching of the uterus: By 9 months, the uterus is stretched to its absolute maximum limit by the baby and the fluid, causing it to naturally want to contract and empty itself.
- Pressure on the cervix: The heavy baby's head presses down on the nerve endings in the cervix (the cervical ganglion). This nerve pressure sends a message to the brain to start labour.
- Braxton Hicks strength: The constant increase in the strength and frequency of practice contractions eventually blends into true labour.
The Stages of Labour
Normal labour is divided into four distinct stages to help midwives monitor the mother safely:
1. First Stage (Stage of Cervical Dilatation)
This stage begins with the onset of regular, rhythmic uterine contractions and is complete when the cervix is fully open (dilated to 10cm). It is broken down into three phases:
- Latent phase: A slow period where the cervix opens from 0 to 3cm. In mothers having their first baby, this slow phase can take 6 to 8 hours.
- Active phase: The cervix begins to open much faster. This phase starts when the cervix is 4cm dilated and ends when it reaches 8cm.
- Transitional phase: The hardest and final part of the first stage. It starts at 8cm and ends when the cervix is fully dilated (10cm).
2. Second Stage (Stage of Expulsion)
This is the stage where the baby is actually pushed out. It begins when the cervix is fully dilated and ends when the baby is completely born. It has two phases:
- Propulsive phase: The baby's head descends from the fully opened cervix down onto the pelvic floor muscles.
- Expulsive phase: The mother feels a strong, uncontrollable urge to push (bear down). This phase ends with the actual delivery of the baby.
3. Third Stage (Placental Stage)
This stage begins immediately after the birth of the baby and ends with the complete separation and expulsion of the placenta and membranes. It involves controlling the mother's bleeding. Naturally, it takes 5 to 30 minutes, but with active management by a midwife, it is usually completed within 5 to 15 minutes.
4. Fourth Stage (Recovery Stage)
This is the critical observation period. It is defined as the first one hour immediately after the placenta is delivered. The midwife closely monitors the mother for bleeding and checks her vital signs to ensure she is recovering well.
💡 Quick Practice Check
Question: A pregnant mother comes to the ward complaining of abdominal pain. Upon assessment, you notice she is having painful contractions, but her cervix is completely closed (0cm dilated), and the pain stops when you advise her to walk around. What is she experiencing?
Answer: False Labour. The key signs are no cervical dilatation, and the pain reduces with movement.

Good work thanks 🙏🙏
Very good work
Well explained
Good work done
Wow thanks a lot may God bless u🙏
Thank you 🙏🙏
Very good work, well explained