MALE INVOLVEMENT IN REPRODUCTIVE HEALTH SERVICES
Male involvement is having men participating more in Reproductive health matters as clients and partners.
This can be in the form of seeking and sharing reproductive health information and services with their partners and friends. Sharing domestic chores and child rearing responsibilities is another form of male involvement, joint decision-making between men and their partners will improve the utilization of family planning, STI and EMTCT services.
Male involvement is embedded in the International Conference on Population and Development Program of Action which includes male responsibilities and participation as critical aspects for improving reproductive health outcomes, achieving gender equality, equity and empowering women. This mandate contributes to broadening the concept of gender so that it now includes men.
Male involvement is critical in the reduction of maternal and infant mortality and morbidity in Uganda. Culturally men are the decision-makers in Uganda. Many women are not empowered (decision and economically) to seek health care without consulting their spouses. Some recognize danger signs during or puerperium but wait for their spouses to return home and consent to their seeking for health care. The decision on where to seek care primarily depends on the spouse and his relatives. Evidence from maternal death audits shows that this delay has contributed to the high maternal and infant mortality and morbidity rates in Uganda.
- Decisions to keep the family healthy and seek care involve gender power roles
- Where men control household resources indirect costs of care seeking are at their discretion
- Control of STDs/HIV is a key R.H issue for men, who are often involved in high risk behaviour
- Decision on number of children is often dictated by men
- SRH issues involve an emotional journey and both men women need the emotional support
- Since men control the resources, women often have to explain why they have go to facilities
- Preventive services are often harder to justify than emergencies that men need in equal measures are inaccessible to them
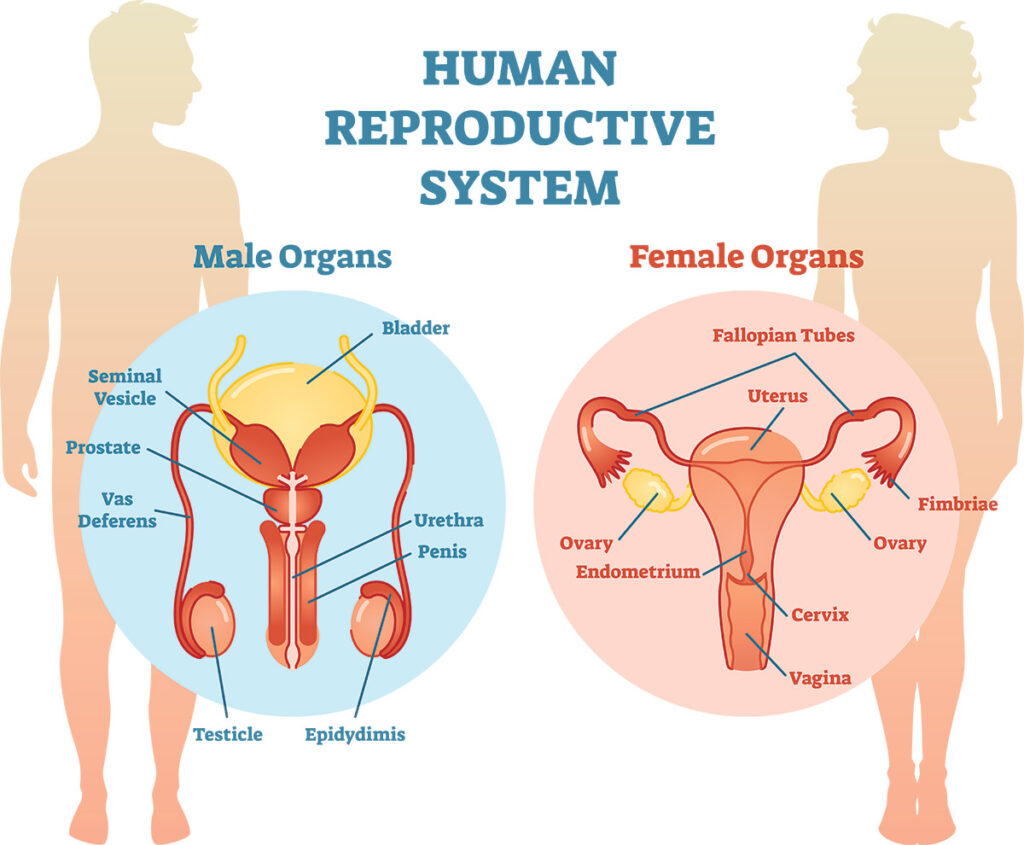
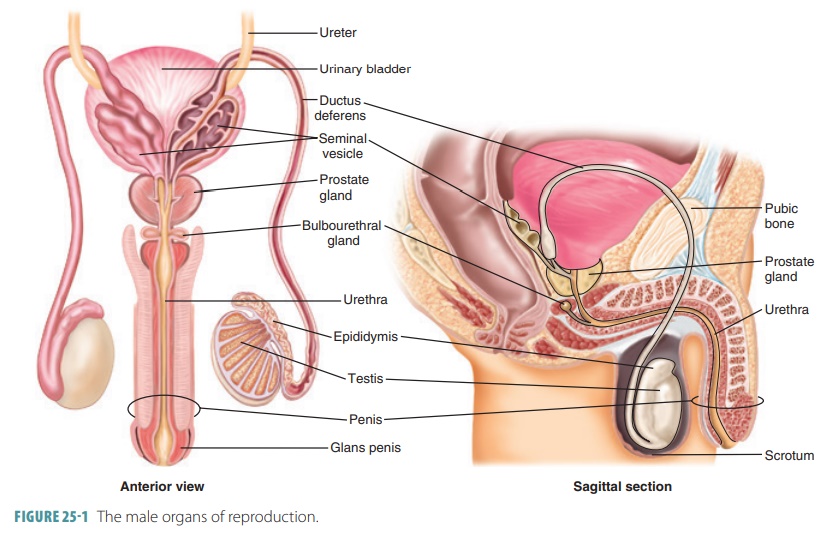
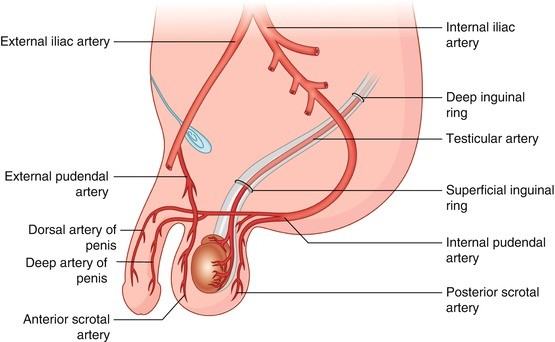
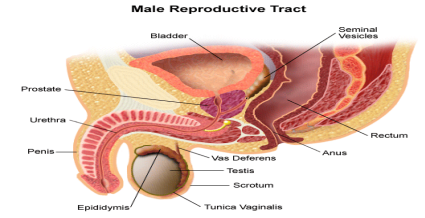
Men have sexual and reproductive health problems which need to be addressed. Conditions of the male reproductive system including; – HIV/AIDs, fertility problems, midlife concerns, such as andropause and sexual dysfunction. Serious conditions include non- malignant genitor-urinary conditions and malignancies of prostate, testicles and genitor-urinary organs.
Vulnerability of males to SRH problems, their roles and responsibilities in prevention and care, including the prevention of gender based violence, are important aspects of a gendered approach to prevention interventions. Empirical and anecdotal evidence indicates that often, cultural beliefs and expectations of manhood or masculinity encourage risky behaviour in men. Masculinity requires males to play brave by not seeking help or medical treatment if they are faced with ailments including HIV/AIDs. Violence against women is more common and arises from the notion of masculinity based on sexual and physical domination over women. Gender based violence is a cross-cutting issue in all the sectors, exists within family and community spaces, and is entrenched within the existing ethno-cultures and its consequences are grave.
In the past, men’s involvement has sometimes been opposed by women’s health advocates, who understandably fear that adding these services will damage the quality of women’s services and create additional competition for already scarce resources. However, adding programs for men can enhance rather than deplete existing programs if the designers of these programs carefully integrate them into the existing health care structure in a way that benefits both women and men.
Both the 1994 International Conference on Population and Development in Cairo and the 1995 Fourth World Conference on Women in Beijing endorsed the incorporation of reproductive health services that include men, mandating that men’s constructive roles be made part of the broader reproductive health agenda.
In fact, neglecting to provide information and services for men can detract from women’s overall health. For example, men who are educated about reproductive health issues are more likely to support their partners in decisions on contraceptive use and family planning, support that may be essential if women are to practice safe sex or avoid unwanted pregnancy. Moreover, if men are knowledgeable about reproductive health issues and can communicate about them with their partners, they are more likely to be supportive during pregnancy and may make better health care decisions: for example, by ensuring that their partner receives emergency obstetric services when needed, rather than delaying recourse to such care. The effect of men’s attitudes and behavior on women’s health is perhaps most obvious in regard to the pandemic of AIDS and other STDs. Programs that educate, test and treat only one partner will not be effective in safeguarding the continued health of both. Men need to share the responsibility of disease prevention, as well as the risks and benefits of contraception.