
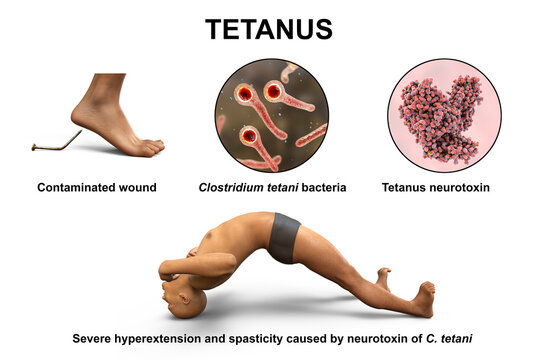

Management of Tetanus
There’s no cure for tetanus. A tetanus infection requires emergency and long-term supportive care while the disease runs its course.
Aims of Management
- To control spasms.
- To eliminate the causative organism and its toxins.
- To prevent complications, and ensure adequate nutrition for the patient.
Specific treatment measures include:
Penicillin: Administering penicillin is a crucial step in destroying the tetanus-causing organism.
Anti-tetanus serum: The administration of anti-tetanus serum helps neutralize the spreading toxins and halt their further detrimental effects.
Sedation and muscle relaxants: Medications like diazepam and chlorpromazine are given to provide sedation and muscle relaxation, effectively alleviating spasms and minimizing discomfort.
Wound management: If there is a wound or focus of infection where the tetanus bacteria may have entered, the dead tissue is excised, and the area is irrigated with hydrogen peroxide. Leaving the wound open without suturing promotes oxygen exposure, hindering the growth of tetanus bacilli, which thrive in anaerobic conditions.
Neutralizing the Toxin:
- Tetanus Immunoglobulin (TIG): Human TIG is administered to neutralize circulating toxins. The dose varies depending on age and the severity of the contamination:
- Adults and children: 150 IU/kg (administered at least in two different IM sites, separate from the tetanus toxoid injection site).
- Neonates: 500 IU IM (in at least two different IM sites).
Tetanus Toxoid (TT) or DPT: The appropriate vaccine (TT or DPT) should be administered immediately to provide active immunity. Refer to the vaccination guidelines for specific age-appropriate regimens.
Eliminating the Source of Toxin:
- Wound management: Thorough cleaning and debridement of wounds to remove necrotic tissue and eliminate the bacterial source. For umbilical wounds in neonatal tetanus, meticulous cleaning and debridement of the umbilical stump are essential.
Antibiotic Treatment:
- First-line: Metronidazole (500 mg every 8 hours IV or orally for 7 days; children: 7.5 mg/kg every 8 hours).
- Second-line: Benzylpenicillin (2.5 MU every 6 hours for 10 days; children: 50,000-100,000 IU/kg per dose; Neonates: 100,000 IU/kg every 12 hours for 10-14 days)
Control of Muscle Spasms:
- First-line: Diazepam (10 mg IV or rectal every 1-4 hours; children: 0.2 mg/kg IV or 0.5 mg/kg rectal every 1-4 hours, max 10mg). For Neonates: 0.2 mg/kg IV or 0.5 mg/kg rectal every 1 to 4 hours.
- Other agents: Magnesium sulfate (alone or with diazepam), chlorpromazine (alone or alternating with diazepam). Monitor for side effects (e.g., respiratory depression with diazepam, loss of knee-jerk reflex with magnesium sulfate). Chlorpromazine dosage for neonates: 1 mg/kg orally 8 hourly via NGT.
Pain Control:
- Morphine: (2.5-10 mg IV every 4-6 hours; monitor for respiratory depression; children: 0.1 mg/kg per dose).
- Paracetamol: (1 g every 8 hours; children: 10 mg/kg every 6 hours).
Prevention:
- Routine childhood immunization: All children should receive the recommended tetanus toxoid-containing vaccines (DTP, Tdap, or Td) as per national immunization schedules.
- Proper wound care: Prompt and appropriate treatment of wounds, including cleaning and debridement, significantly reduces the risk.
- Prophylactic TIG: For individuals with contaminated wounds and incomplete or unknown immunization status:
- Children < 5 years: 75 IU
- Children 5-10 years: 125 IU
- Children > 10 years and adults: 250 IU
Wound care: Proper care of wounds, including thorough cleaning and debridement, helps prevent infection.
Control of spasms involves the following measures:
- Absolute rest and isolation: The patient should be kept in a quiet room with dim lighting to minimize triggers for spasms.
- Prevention of external stimuli: Measures such as fitting the door with suitable closing materials or springs prevent slamming noises that could stimulate the patient.
- Warming hands before touching: Nurses should warm their hands before touching the patient to avoid any stimulation that might trigger spasms.
- Medication administration: Sedatives and muscle relaxants, such as chlorpromazine (Largactil), and Diazepam, are given regularly through a nasogastric tube to maintain a controlled state and alleviate spasms.
o Example of 6 hourly regimen
Drug
6-9
am
9-12
pm
12-3
pm
3-6
pm
6-9
pm
9-12
am
12-3
am
3-6
am
6-9
am
Largactil

⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
Diazepam
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼
⫼⫼⫼⫼

It making learning interesting
It was interesting reading about tetanus.
So interesting
Soo interesting, thanks
so educative
Wow so marvelous
grateful for the knowledge 🙏
wow so educative
Needs to be a bit compiled
Wow, the work is simplified