
Tuberculosis (TB) & New National Management Guidelines
1. Aetiology and Mode of Spread
Aetiology (Cause of the Disease)
The primary causative organism for this disease is Mycobacterium tuberculosis (also known as the Tubercle Bacillus). It is a small, aerobic (requires oxygen to survive), non-motile (cannot move on its own) bacillus (rod-shaped bacterium).
Mode of Spread (Transmission)
Tuberculosis is highly contagious and spreads through multiple pathways:
- Airborne Droplet Infection: The bacteria spread rapidly through the air when an individual with an active, untreated pulmonary TB infection coughs, sneezes, speaks, or sings. This releases invisible respiratory fluids containing the bacilli into the air.
- Haematogenous Spread: Once inside the body, the bacteria can enter the bloodstream and spread to distant organs.
- Close Contact: Prolonged, frequent, or intense contact with a person who has infectious TB (such as living together or spending a great deal of time in close proximity).
- Zoonotic TB: Though less common today, Mycobacterium bovis can be transmitted through consuming unpasteurized milk or direct contact with infected cattle/abattoir environments.
2. Classification and Types of Tuberculosis
Tuberculosis is broadly classified based on the site of infection, the patient's exposure history, and its resistance to medications:
- Pulmonary Tuberculosis (PTB): TB strictly affecting the lungs. It is the most common and the only highly infectious form.
- Extra-Pulmonary Tuberculosis (EPTB): TB affecting organs outside the lungs (e.g., bones, brain, lymph nodes). It is generally not infectious to others.
- Primary Tuberculosis: The very first time a person is exposed to and infected with the TB bacteria.
- Secondary Tuberculosis: A reactivation of a dormant TB infection or a massive new reinfection from the environment.
- Latent TB Infection (LTBI): The bacteria are alive but inactive (sleeping) inside the body. The patient has no symptoms, does not feel sick, cannot spread the disease, but tests positive on skin or blood tests.
Drug-Resistant TB (DR-TB) Classifications
According to WHO and National Guidelines, DR-TB occurs when bacteria survive despite the use of standard medicines. It is classified as:
- Mono-resistant TB: Resistance to exactly one first-line anti-TB drug.
- Poly-resistant TB: Resistance to more than one first-line drug (but NOT both Isoniazid and Rifampicin together).
- Rifampicin-Resistant TB (RR-TB): Resistance specifically to Rifampicin, detected with or without resistance to other drugs. Treated identically to MDR-TB.
- Multidrug-Resistant TB (MDR-TB): Resistance to at least both Isoniazid and Rifampicin, the two most powerful first-line drugs.
- Extensively Drug-Resistant TB (XDR-TB): MDR-TB plus additional resistance to any Fluoroquinolone and at least one Group A drug (like Bedaquiline or Linezolid).
3. Clinical Features (Signs and Symptoms)
A. Pulmonary TB
Patients with active lung TB classically present with:
- Persistent Cough: Lasting for more than 2 to 3 weeks. It may be productive (with thick sputum) or a non-productive, dry cough.
- Haemoptysis: Coughing up fresh blood or blood-stained sputum due to severe lung tissue destruction.
- Fever and Chills: Usually a low-grade fever that peaks in the late afternoon or evening.
- Night Sweats: Profuse, drenching sweating during sleep.
- Weight Loss & Anorexia: Severe loss of appetite resulting in noticeable, unexplained body wasting.
- Easy Fatigability: Extreme weakness and lack of energy.
- Chest Pain: Pain while breathing or coughing due to pleural involvement.
- Finger Clubbing: Abnormal swelling and rounding of the fingertips, caused by chronic lack of oxygen (hypoxia) over a long period.
B. Extra-Pulmonary TB (EPTB)
In approximately 15-20% of active cases (and over 50% in HIV+ patients), the bacilli escape the lungs. Notable sites include:
- The Pleura: Causes Tuberculous Pleurisy (fluid and inflammation around the lungs).
- Central Nervous System (CNS): Causes Tuberculous Meningitis, a highly fatal swelling of the brain lining.
- Lymphatic System: Causes swollen, matted TB lymph nodes (often in the neck, historically called Scrofula).
- Genitourinary System: Causes Urogenital Tuberculosis, affecting the kidneys and reproductive organs.
- Bones and Joints: Known as Osseous Tuberculosis or TB Osteomyelitis. When it destroys the spine, it is called Pott’s Disease.
- Skin: A deep tubercular abscess can burst through the skin, forming a painless, discharging Tuberculous Ulcer.
⚠️ Clinical Alert: Miliary Tuberculosis
This is a severe, widespread, and life-threatening form of TB. It happens when massive amounts of bacteria enter the bloodstream and spread everywhere, forming tiny "millet-seed" sized white spots all over the body's internal organs. Miliary TB accounts for about 10% of extra-pulmonary cases and is highly common in young children and immunocompromised patients.
4. Epidemiology and High-Risk Populations (Uganda Context)
Epidemiology (2024/2025 Data)
- Global: Approximately one-third of the global population is infected with dormant TB. Africa has the world's highest incidence rate.
- Uganda Incidence: Uganda is among the 30 high TB and TB/HIV burden countries globally. The incidence is 198 cases per 100,000 population, equating to about 96,000 new cases annually.
- Missed Cases: Despite progress, approximately 20,000 TB cases remain undiagnosed annually in Uganda.
- Demographics: Men account for ~64% of cases. Children (0-14 years) account for 13.8% of notifications.
- Co-infection & Mortality: The TB/HIV co-infection rate is dangerously high at 37%. TB causes roughly 15,000 deaths annually in Uganda.
High-Risk and Vulnerable Populations
Uganda's National Strategy heavily prioritizes active case finding in the following groups:
- People in Prisons: Prevalence is alarmingly high at 1,904 per 100,000 (nearly 8 times the national average), heavily driven by overcrowding and poor ventilation.
- People Living with HIV (PLHIV): HIV is the most significant global risk factor, weakening the immune system and driving the rapid progression of active TB.
- Children under 5 & Adolescents: Highly vulnerable to severe forms like meningitis and miliary TB. Contact tracing is crucial.
- Men: Men have a higher prevalence but poor health-seeking behavior, leaving many undiagnosed and untreated.
- Other Key Populations: Urban slum dwellers, miners, pastoralists, refugees, healthcare workers, tobacco smokers, and people with diabetes or severe undernutrition.
5. Pathogenesis: The Cellular Process
Primary Tuberculosis
- The bacilli are inhaled deep into the lung air sacs (alveoli), where they invade macrophages, replicate, and trigger an inflammatory response.
- They travel through the lymphatic system to the hilar lymph nodes (nodes in the center of the chest).
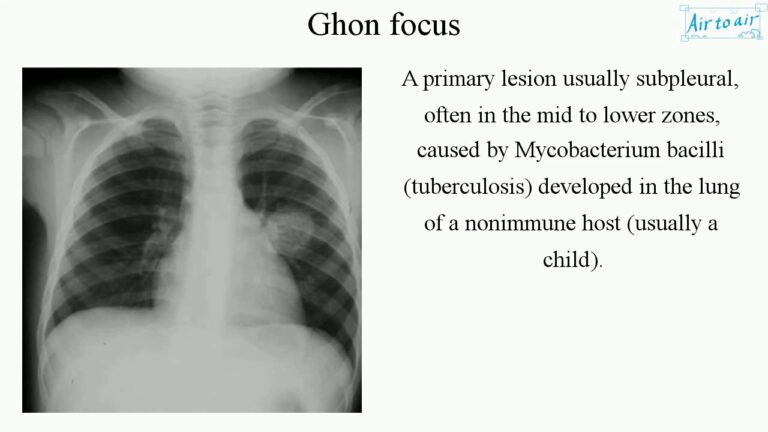
- About 6 weeks after infection, the body’s immune system wakes up. The bacilli are surrounded and "walled off" by specialized immune cells (macrophages, T and B lymphocytes, fibroblasts, and epithelioid cells).
- This hard, trapped nodule in the lung is called a Ghon Focus.
- The combination of the Ghon Focus and the swollen hilar lymph nodes is called the Primary Complex.
- In 90% of people, the bacteria stay asleep inside this wall for years (Latent TB).
Secondary Tuberculosis & Caseation
- Occurs due to reactivation of dormant bacilli (when immunity drops) or massive reinfection.
- Inside the immune walls (Granulomas), abnormal cell death occurs. The center turns into a soft, white, cheese-like substance. This is called Caseation Necrosis.
- Tissue destruction and necrosis are balanced by healing and fibrosis. If the bacteria win, they dissolve the lung tissue, leaving large empty holes called Cavities filled with highly infectious caseous material.
6. Diagnosis and Investigations (Modern Guidelines)
Uganda's current standard of care has aggressively shifted away from basic microscopy towards Universal access to Molecular WHO-Recommended Rapid Diagnostics (mWRDs).
| Diagnostic Tool | Clinical Application & Modern Strategy |
|---|---|
| GeneXpert / TrueNat (mWRDs) | The absolute first-line test. GeneXpert Ultra machines rapidly detect both the TB DNA and Rifampicin resistance (RR-TB) simultaneously. The goal is 100% molecular testing. |
| Digital Chest X-Ray (dCXR) with CAD/AI | Used heavily for screening, especially in mobile vans and high-risk populations. Computer-Aided Detection (CAD) Artificial Intelligence helps automatically flag abnormal infiltrates, cavities, or nodules. |
| Urine LF-LAM | A specialized rapid test using urine. Highly effective and specifically indicated for screening TB in PLHIV with advanced disease (very low CD4 counts). |
| Stool Testing | An alternative specimen collection method now recommended for Childhood TB, as children swallow their sputum and cannot expectorate easily. |
| Culture & Second-Line DST | Samples are referred to the National TB Reference Laboratory (NTRL) to grow the bacteria and perform comprehensive Drug Susceptibility Testing (DST), including Line Probe Assays (LPAs) and Next Generation Sequencing (NGS) for MDR/XDR-TB. |
| Sputum Microscopy (AFB) | Still available but now primarily used for treatment follow-up to see if the patient is converting to negative, rather than initial diagnosis. |
| Tuberculin Skin Test (Mantoux) | Used to assess Latent TB Infection (LTBI), especially in children and healthcare workers. |
7. The Relationship Between HIV and TB Co-Infection
HIV and Tuberculosis are deeply connected. They act together in a deadly cycle where each disease makes the other much worse. Understanding their relationship is critical for a midwife managing infectious diseases.
A. Effects of HIV on Tuberculosis
HIV severely weakens the immune system (destroying CD4 cells), which changes how TB behaves in the body:
- Development of active TB: Individuals infected with HIV have a much higher risk of developing active tuberculosis once they are exposed to the TB bacteria, instead of keeping it dormant.
- High risk of re-infection: HIV-positive individuals are highly susceptible to being infected with a brand new, second strain of TB from the environment, even after they have already had the infection and been treated.
- Increased incidence of TB: The overall number of tuberculosis cases in the population increases greatly due to the high prevalence of HIV, which weakens the community's immune defenses and makes individuals far more susceptible to catching TB.
- Changes in TB presentation: TB in HIV-positive individuals often presents with completely different clinical and bacteriological signs. Because the immune system cannot form cavities to fight the bacteria, patients may have a non-productive (dry) cough, a total absence of hemoptysis (no coughing up blood), and X-rays will show a scattered miliary pattern instead of the typical large lung cavitations.
- Quicker development of TB complications: HIV acts as an accelerator, speeding up the progression of TB disease and causing severe complications much faster than in an HIV-negative person.
B. Effects of Tuberculosis on HIV
- Increased HIV replication: TB infection causes massive inflammation in the body. This immune response actually enhances and speeds up the replication of the HIV virus, leading to a much higher viral load and a faster progression into full-blown AIDS.
- Common opportunistic infection: TB is one of the most frequent opportunistic infections to attack individuals living with HIV. It stands as the leading cause of death in this vulnerable population.
- Interference with ARV treatment: Strong anti-TB medications, specifically Rifampicin, can heavily interfere with certain antiretroviral drugs (ARVs), such as Nevirapine and Protease Inhibitors. This dangerous drug-to-drug interaction necessitates expert adjustments in the patient's treatment plan.
C. Consequences of Dual Infection (Having both HIV and TB)
- Increased morbidity and mortality: Patients suffer much higher rates of severe sickness and death.
- Higher recurrence rate: There is a higher chance of the TB coming back even after successfully completing a full course of treatment.
- Drug resistance: Dual infection often leads to poor drug absorption and resistance, resulting in dangerous Multidrug-Resistant TB (MDR-TB) and Extensively Drug-Resistant TB (XDR-TB).
- Higher rates of treatment non-adherence: Because the patient has to swallow so many pills for both HIV and TB (overlapping medication regimens), they often get tired and stop taking their drugs.
- Increased risk of drug toxicity: Taking strong TB drugs and ARVs at the same time heavily stresses the liver and kidneys, leading to severe toxic side effects.
⚠️ Management of HIV and TB Co-infection
When a patient has both diseases, the timing and management of their medications must follow strict clinical guidelines:
- Prioritize TB Treatment First: Always start treating the Tuberculosis before starting the ARVs to prevent deadly immune reactions.
- Timing of ARVs: Start ARVs if the patient's CD4 count is below 350 cells/mm³. This is usually done either immediately after finishing TB treatment or carefully during the intensive phase of TB treatment, depending on the patient's exact clinical situation.
- Manage Drug Interactions: Carefully consider the chemical interactions between TB drugs (like Rifampicin) and HIV regimens when selecting the final medications.
- Use DOTS: Strictly use Directly Observed Therapy (DOTS) for the TB treatment and monitor the patient very closely for signs of organ toxicity and to ensure absolute adherence.
- Administer Prophylaxis: Give prophylactic drugs (like Cotrimoxazole/Septrin) to prevent other opportunistic infections as indicated.
Complications of Tuberculosis
If TB is not diagnosed early or treated completely, the bacteria will physically destroy the body's tissues, leading to severe, life-threatening complications:
- Pleural effusion: The abnormal and dangerous accumulation of fluid in the pleural space (the thin lining surrounding the outside of the lungs), which crushes the lung and makes breathing extremely difficult.
- Pericardial effusion: The abnormal accumulation of fluid in the sac surrounding the heart, which squeezes the heart muscle and prevents it from pumping blood properly.
- Empyema: The fluid in the pleural space becomes infected and turns into a thick, highly toxic, pus-filled cavity.
- Pneumothorax: The TB bacteria eat through the lung tissue, allowing air or gas to leak out into the pleural cavity. The trapped air builds pressure, causing the lung to completely collapse.
- Lung fibrosis: Heavy, permanent scarring and stiffening of the delicate lung tissue, leading to permanently impaired lung function and lifelong breathing problems.
- Lung collapse: The collapse of an entire lung or just a part (lobe) of a lung due to severe blockage of the airways or compression from outside fluid/air.
- Extra-pulmonary TB: The TB bacteria escape the lungs and aggressively attack other vital organs. A prime example is TB Meningitis, where the bacteria attack the lining of the brain and spinal cord, which is frequently fatal.
8. Complications of Untreated TB
- Pleural Effusion: A massive accumulation of fluid in the pleural space, crushing the lungs.
- Empyema: The fluid in the pleural cavity turns into a thick, toxic pocket of pus.
- Pericardial Effusion: Fluid building up in the sac around the heart, restricting its ability to pump.
- Pneumothorax: Lung tissue is destroyed, leaking air into the chest cavity and causing lung collapse.
- Lung Fibrosis & Post-TB Lung Disease (PTLD): Heavy, permanent scarring of the lung tissue. Uganda guidelines now emphasize assessing Quality of Life post-treatment and linking patients with PTLD to pulmonary rehabilitation.

9. Treatment and Management Guidelines
Aims of TB Treatment
- To completely cure the patient (achieve >95% Treatment Success Rate).
- To prevent complications, death, and Post-TB disabilities.
- To rapidly reduce the transmission of TB to the community.
Standard TB Treatment Regimens (The Shift to Shorter Courses)
Uganda is actively updating regimens based on the latest WHO evidence to improve adherence and reduce patient costs.
| Patient Category | Modern Treatment Strategy & Regimen Notes |
|---|---|
| Drug-Susceptible TB (DS-TB) - Adult | Standard 6-month regimen (2HRZE / 4HR). However, the NSP mandates scaling up and evaluating new shorter 4-month DS-TB regimens to improve completion rates. |
| Childhood TB (DS-TB) | Scale up the use of shorter child-friendly regimens (4-month regimens) and ensure the uninterrupted supply of optimized pediatric FDCs (Fixed Dose Combinations). |
| MDR-TB / RR-TB | Aggressive expansion of decentralized care using shorter, all-oral regimens (e.g., BPaLM / BPaL). This avoids painful daily injections, reduces toxicity, and has pushed DR-TB success rates to 88%. |
🧠 Memory Trick: The Core First-Line Anti-TB Drugs
Remember the acronym STRIPE:
- S - Streptomycin (S)
- T - (often substituted or dropped in modern oral regimens, but part of historical first-line)
- R - Rifampicin (R)
- I - Isoniazid (H or INH)
- P - Pyrazinamide (Z)
- E - Ethambutol (E)
*Note: Pyridoxine (Vitamin B6) is always co-administered with Isoniazid to prevent peripheral neuropathy (nerve damage). Corticosteroids (Steroids) are added for severe inflammation like TB Meningitis or Pericarditis.
Socio-Economic Support & Catastrophic Costs
A major focus of modern TB management is protecting the patient's finances. Over 53.1% of TB-affected households face catastrophic costs (spending >20% of their annual income on transport, nutrition, and hidden fees). The strategy mandates:
- Providing Enabler Packages (food rations, transport vouchers, cash transfers).
- Linking patients to social protection schemes (PDM, SAGE).
- Removing all patient fees for Chest X-rays in public facilities and reimbursing private facilities to offer them free of charge.
10. DOTS, Digital Health, & Community Prevention
Modernizing DOTS (Directly Observed Therapy)
While traditional DOTS relies on a trained worker physically watching the patient swallow pills, Uganda is rapidly scaling up Digital Adherence Technologies (DATs):
- Smart Pill Boxes: Boxes that log exactly when the patient opens them.
- Video DOT (VDOT): Patients record themselves taking medication via smartphone, allowing remote monitoring.
- DSD Models: Differentiated Service Delivery allows stable patients to receive fast-track community refills rather than traveling long distances to the clinic daily.
Preventive Treatment (TPT) & Contact Tracing
- TB Preventive Treatment (TPT): Giving prophylactic drugs (like 1HP, 3HP, 3HR) to high-risk groups to stop Latent TB from becoming active. The target is 95% coverage for children under 5, PLHIV, and household contacts.
- Contact Investigation: Systematically tracing, line-listing, and screening every person living in the household of a confirmed TB patient.
- Multisectoral Accountability Framework (MAF-TB): Engaging non-health sectors. Examples include the Ministry of Education enforcing school ventilation, Ministry of Internal Affairs screening prisoners, and the Ministry of Transport enforcing ventilation in taxis to prevent airborne spread.
📝 Quick Review
Question: Why is the national strategy heavily pushing for the adoption of Digital Adherence Technologies (DATs) like Video DOT (VDOT) and Smart Pill Boxes?
- Answer: Because TB treatment is very long. DATs reduce the catastrophic transport costs for patients who previously had to travel to the clinic daily, while still allowing the midwife/health system to guarantee the patient is taking their medication, preventing drug resistance (MDR-TB).
11. References
- World Health Organization (WHO) Guidelines for Treatment of Tuberculosis.
- Uganda Ministry of Health (MoH) National Tuberculosis and Leprosy Programme (NTLP) Manual.
- UNMEB Curriculum for Diploma in Midwifery/Nursing - Tropical Medicine & Medical Disorders.

Thanks for the assistance it’s great
The notes are so helpful for revision
Complex topics made easier to understand, thank you very much.
Thank you for the revision notes.
Very good notes and easy to understand
good