
Table of Contents
TogglePHYSIOLOGY OF PREGNANCY
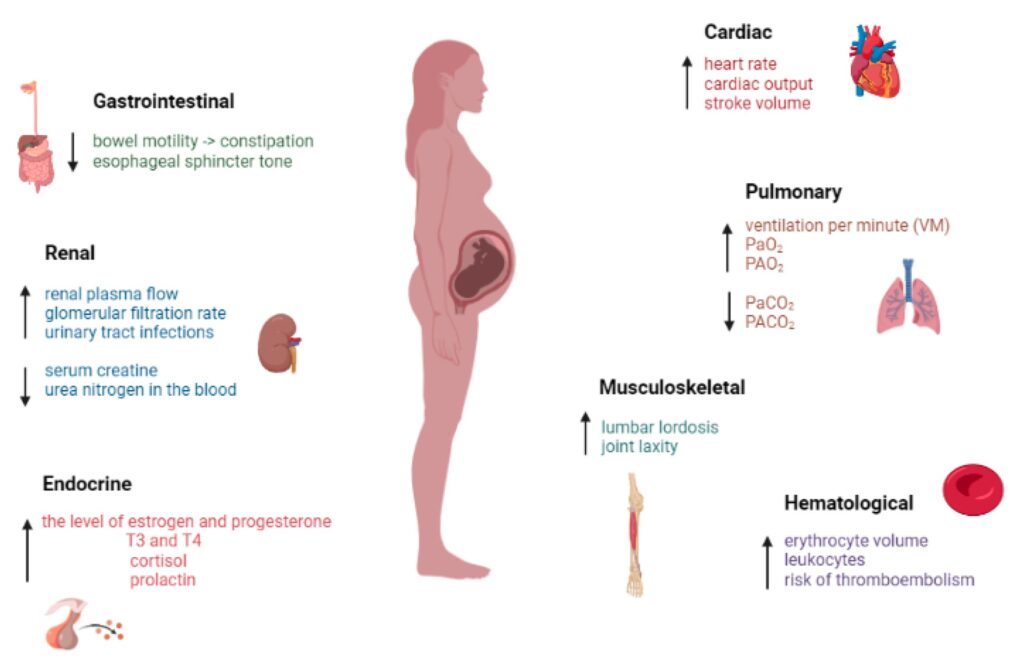
These are normal natural changes that occur in the body due to pregnancy. These result mainly from alteration of hormones and metabolism.
CHANGES IN THE ENDOCRINE SYSTEM
- Hormonal changes:
The placenta produces several hormones which cause a number of physiological changes.
Successful physiological adaptation of pregnancy is due to alterations in hormone production by the maternal endocrine system and the trophoblast. - Human chorionic gonadotrophic hormone.
It is produced by the trophoblast. H.C.G levels increase rapidly in early pregnancy, maximum levels being attained at 8-10 weeks of gestation. The main function of HCG is to maintain the
corpus luteum in order to ensure secretion of progesterone and Oestrogen until placental production is adequate after 10-12 weeks after which concentration of HCG gradually decreases until it has completely disappeared 2 weeks after birth. - Progesterone hormone;
This is produced mainly in the corpus luteum. Its function is to thicken the decidua in order to receive a fertilized ovum. It helps to increase the glandular tissue, ducts of the breasts and muscle
fibres of the uterus. - Oestrogen;
It causes growth of the uterus and duct system of the breasts in pregnancy. It is excreted in urine and amount present indicates fetal wellbeing. - Relaxin hormone;
During the last weeks of pregnancy, it acts on ligaments and joints producing the “give” of the pelvis. It is also produced by decidua and the trophoblast to promote myometrium relaxation and
may play a role in cervical ripening and rapture of membranes. - HPL ( human placental lactogen): It stimulates the growth of breasts and has lactogenic properties that affect a number of metabolic changes. These changes brought about by HPL ensure that glucose is readily available for body and brain growth in the developing fetus, and protects against nutritional deficiencies.
- Pituitary hormones: The follicle stimulating hormone and L.H are suppressed by the high levels of Oestrogen and progesterone. The adrenal gland increases only slightly in size during pregnancy due to hypertrophy and widening in glucocorticoid area which suggests increased secretion of hormones.
- Thyroid function: In normal pregnancy, the thyroid gland increases due to hyperplasia of glandular tissue and increased vascularity. There is normally an increased uptake of iodine during pregnancy which may be to compensate for renal clearance of iodine leading to reduced level of plasma iodine.
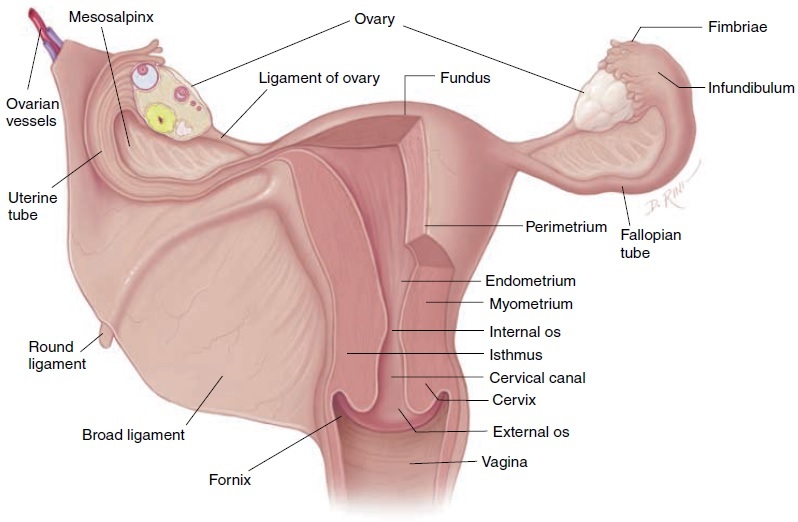
CHANGES IN THE REPRODUCTIVE SYSTEM
CHANGES IN THE UTERUS:
It stretches and expands to accommodate and nurture the growing fetus. This occurs in the
myometrium. The body grows to provide a nutritive and protective environment in which the fetus will develop and grow.
Uterine muscle layers;
1. Endometrium;
– Menstruation stops.
-It becomes the decidua during pregnancy.
-It becomes thick, soft, spongy and readily supplied with blood.
2 . Myometrium.
- The enlargement of the body of the uterus is due to 2 factors.
1. The actual muscle fibres enlarge increasing in length about 10 times and in width about 3 times.
This process is called hypertrophy (increase in size).
2. The new muscle cells make their appearance and grow alongside the original muscle cells. This process is called hyperplasia (increase in number).
The size; as pregnancy advances, the uterus grows from its normal size. The length being 7.5cm,
width 5cm and thickness 2.5cm. So it becomes 30cm in length, 23cm in width and 20 cm in
thickness. The weight increases from 60g to 960g.
The shape; Health growth of the uterus requires adequate space to accommodate the growing fetus, increasing amount of liquor and placental tissue. After conception, the uterus enlarges
because of Oestrogen. At the beginning of pregnancy, it is pear shaped organ, at the end of 12 weeks, it is globular, from 12-38weeks its oval shaped and when lightening takes place after 38weeks, it turns back to globular.
Muscle layers of the myometrium;
- Outer most longitudinal layer,
This layer begins in the anterior wall of the upper uterine segment, passes over the fundus and down the posterior wall. It is by contraction and retraction of this muscle layer that the fetus is expelled from the uterus during labour. - Middle oblique layer,
In this case, muscles are arranged in criss cross manner; the muscle cells surround the blood vessels in the figure of 8 pattern. After separation and expulsion of the placenta, they compress the blood vessels and help to prevent PPH. They are sometimes referred to as living ligatures. - Inner circular layer,
This is the weakest of the 3 layers, the muscle fibres pass transversely around the uterus. They are more developed around the cervix, lower uterine segment and the fallopian tubes. They help in cervical dilatation.
3. The perimetrium;
This is the layer of the peritoneum which does not totally cover the uterus, its deflexed over the bladder anteriorly to form the utero vesicle pouch and posteriorly forming pouch of Douglas. After 12 weeks, the uterus rises out of pelvis and becomes an abdominal organ. It loses its ante-version and ante flexed position and becomes erect and leans on its axis on the right.
CLINICAL OBSERVATIONS OF THE GROWING UTERUS
- At 12 weeks
The uterus is out of the pelvis and becomes upright; it is no longer anteverted and ante flexed. The uterus is palpable just above the symphysis pubis and is about the size of a grape fruit.
- At 16 weeks
Between 12 and 16 weeks, the fundus becomes dome shaped. As it rises, it rotates to the right (dextrorotation) due to the recto sigmoid colon in the left side of the pelvis and exerts tension on the broad and round ligaments.
The conceptus has grown enough to put pressure on the isthmus causing it to open out so that the uterus becomes more globular in shape.
- At 20 weeks
The fundus of the uterus may be palpated at the level of the umbilicus. The uterus becomes more rounded around the fundus.
- At 30 weeks
The fundus may be palpated midway between the umbilicus and ximphoid sternum. Enlarging uterus displaces the intestines laterally and superiorly. Abdominal wall supports the uterus and maintains the relationship btn the long axis of the uterus and axis of the pelvic inlet.
In supine position, the uterus falls back to the vertebral column, aorta and inferior venacava.
- At 36 weeks
By the end of 36 weeks, the enlarged uterus fills the abdominal cavity. The fundus is at the tip of the ximphoid cartilage.
- At 38 weeks
Between 38 and 40 weeks, there is increase in smoothening and softening of the lower uterine segment. Uterus becomes more rounded with a decrease in fundal height. The reduction in fundal height is known as lightening.
Changes in blood supply: The uterine blood vessels increase in diameter and new vessels develop under the influence of Oestrogen. Blood supply to the uterine and ovarian arteries increases to about 750ml/ min at term to keep pace with its growth and meet the needs of the functioning placenta.
Changes in the fallopian tubes: On either side are more stretched out and are more vascular in pregnancy. Uterine end of the tube is usually closed and fimbriated end remains open.
Changes in the isthmus;
It softens and elongates from 7mm to23mm and forms the lower uterine segment during late pregnancy.
Changes in the ovaries:
The follicle- stimulating hormone {FSH} ceases its activity due to the increased levels of estrogen and progesterone secreted by the ovaries and corpus luteum .This prevents ovulation and menstruation. As the uterus enlarges, the ovaries are raised out of the pelvis. Also both ovaries are enlarged due to increased vascularity and become edematous particularly that containing the corpus luteum.
The corpus luteum enlarges during early pregnancy and may even form a cyst on the ovary. The corpus luteum produces progesterone to help maintain the lining of the endometrium in early pregnancy. It functions until about the 10th and 12th week of pregnancy when the placenta is capable of producing adequate amounts of progesterone and estrogen. It slowly decreases in size and function after the 10th to 12th week.
Changes in the cervix:
It remains tightly closed during pregnancy, providing protection to the fetus and resistance to pressure from above when the woman is in standing position. There is slight growth on the cervix during pregnancy, it becomes softer and this is due to increased vascularity and relaxing effects of hormones.
Under the influence of progesterone racemose glands secrete thicker and more viscous mucus which fills the cervical canal and prevents entry of infection in the uterus. The plug of mucous is called opeculum
Towards the end of pregnancy or at the onset of labour the cervix becomes part of the lower uterine segment, this is called effacement of the cervix. The external os of the cervix also admits a finger. A short softened cervix or os which admits the tip of a figure at term is referred to as ripe cervix.
Changes in the vagina:
The muscle layer hypertrophies and capacity of vagina increases and it becomes more elastic allowing it to dilate during 2 nd stage.
The epithelium becomes thicker with increased desquamation of the superficial cells which increase the amount of normal white virginal discharge known as leucorrhea. The epithelial cells have high glycogen content. The cells interact with Do-derlein’s bacillus and produce a more acidic environment providing extra degree of protection against some organism and increasing susceptibility to others such as candida albicans. The vagina is more vascular and appears violet in colour.
Changes in the vulva:
The vulva appears bluish in colour due to increased vascularity and pelvic congestion.
Breast changes:
-In early pregnancy, breasts may feel full or tingle and increase in size as pregnancy progresses.
-The nipples become more erectile.
– The areolar of the nipples darken and the diameter increases.
– The sebaceous glands become the Montgomery’s tubercles which enlarge and tend to
protrude. They secrete sebum to lubricate the breast throughout pregnancy and breast feeding.
– The surface vessels of the breast become visible due to increased circulation and turns to bluish
tint on the breasts.
-A little clear, sticky fluid(colostrum) may be expressed from the nipples after the 1 st trimester
which later becomes yellowish in colour.
Changes in the cardiovascular system
The heart
Due to increased work load, the heart hypertrophies particularly in the left ventricle. The uterus pushes the heart upwards and to the left. Heart sounds are changed and murmurs are common.
The cardiac output is increased by 40%. The heart rate increases by an average of 15 beats per minute. The stroke volume increases from 64 to about 71mls.
Effect on blood pressure
During the first trimester, blood pressure remains almost constant. BP drops in 2 nd trimester due to hormone progesterone which causes vasodilation. It reaches its lowest level at 16-20 weeks and towards term, it returns to the level of the first trimester. The decrease may lead to fainting.
Supine position should be avoided in pregnancy as it leads to supine hypotensive syndrome due to compression of the inferior venacava thus reducing venous return. Poor venous return in late pregnancy may lead to oedema in lower limbs, varicose veins and hemorrhoids.
Blood flow
Blood flow increases to uterus, kidneys, breasts and skin but not to liver and brain. Utero placental blood flow increases by 10-15% about 75mls per minute at term. Renal blood flow increases by 70-80%.
Blood volume
Increase in blood volume varies according to the size of the woman, number of pregnancies she has had, parity and whether the pregnancy is singleton or multiple.
The total blood volume increases steadily from early pregnancy to reach a maximum of 35 to 45% above the non- pregnant level. A higher circulating volume is required for the following;
-To provide extra blood flow for placental circulation.
-To supply the extra metabolic needs of the fetus.
-To provide extra perfusion of kidneys and other organs.
-To compensate for blood loss at delivery.
-To counterbalance the effects of increased venous and arterial capacity.
Plasma volume
Increases by 40% where the red cell mass decreases by 20%leading to haemodilution (physiological anaemia). These changes begin at 6-8weeks of pregnancy. The acceptable Hb level in pregnancy is 11-12g/dl.
Iron metabolism
Iron of about 1000g is needed. 500g is to increase the red cell mass, 300g to fetus and 200g for daily iron compensation. In normal pregnancy, only 20% of ingested iron is absorbed. The purpose of iron supplementation is to prevent iron deficiency anaemia not to raise Hb level.
Plasma protein
During the 1st 20 weeks of pregnancy, plasma protein concentration reduces due to increased plasma volume. This leads to lowered osmotic pressure leading to oedema of lower limbs seen in late pregnancy. In absence of disease, moderate oedema is termed as physiological oedema.
Clotting factors
Fibrinogen 7,8,9 and 10 increase leading to a change in coagulation time from 12 to 8 minutes.
The capacity of clotting is increased in preparation to prevent PPH after separation of the placenta.
White blood cells.
These are slightly increased during pregnancy, from 700mm to 10500mm during pregnancy and up to 1600mm during labour. The total count cells rises from 8 weeks and reaches a peak at 30 weeks of gestation. This is mainly because of the increase in the number of neutrophils, polymorphs, nucleus, leucocytes, monocytes and granulocytes are active and efficient phagocytes.
Erythrocytes.
They decrease during pregnancy from 4.5million to 3.7million.
HB.
HB concentration falls from 14g/dl; a falling HB is a physiological. The total iron requirements of pregnancy where as a high HB level can be assign of pathology. The total requirements of
pregnancy is averagely 1000g ,about 500gare required to increase the red cells mass and about 300g are transported to the fetus mainly in the last weeks of pregnancy . The remaining 200g are needed to compensate for insensible loss in skin, stool and urine.
RESPIRATORY SYSTEM.
The basal metabolism rate is increased and the volume of air which enters and leaves the lungs during the normal respiration becomes slightly increased. This is because of increased oxygen consumption by the fetus and the work of maternal heart and lungs.
In the late pregnancy the ribs flare out inhibiting the capacity of the thoracic cavity to expand, the enlarging uterus elevates the diaphragm up wards and compresses the lower lobes of the lungs
CHANGES IN THE URINARY SYSTEM
Renal blood flow and glomerular filtration rate increases by 50%.
There is frequency of micturition in early and late pregnancy. Ureters become elongated and kinked due to progesterone hormone and this results into urine stagnation hence increased favor to UTI in pregnancy.
CHANGES IN THE GIT
-The gums become edematous, soft and spongy and may bleed.
-Increased salivation(ptyalism) is common.
-Nausea and vomiting is common in 70% of the cases.
-Changes in taste becoming metallic.
-Craving for abnormal things like soil or plaster known as pica.
-Increased appetite in most women.
-Heart burn due to of stomach content from decreased space by growing uterus.
-There is reduced GIT motility leading to constipation.
Changes in metabolism
– There is increased metabolism to provide nutrients for the mother and fetus.
-Maternal weight, There is continuing weight increase in pregnancy which is an indication of fetal growth.
Weight gain in pregnancy is as follows;-
4kg in the 1 st 20 weeks(0.2kg/week)
8.5kg in the last 20 weeks(0.4kg/week)
12.5kg approximate total.
| Maternal Weight Gain (kg) | Fetal Weight Gain (kg) | Total Weight Gain (kg) | |
|---|---|---|---|
| Uterus | 1 | – | 1 |
| Breasts | 0.4 | – | 0.4 |
| Fat | 3.5 | – | 3.5 |
| Blood Volume | 1.5 | – | 1.5 |
| Extracellular Fluid | 1.5 | – | 1.5 |
| Fetus | – | 3.4 | 3.4 |
| Placenta | – | 0.6 | 0.6 |
| Amniotic Fluid | – | 0.6 | 0.6 |
| Total | 7.9 | 4.6 | 12.5 |
The following factors influence weight gain during pregnancy:
Maternal oedema: Edema, or swelling, can affect weight gain as it involves the accumulation of excess fluid in the tissues of the body.
Maternal metabolic rate: The metabolic rate of the mother can impact weight gain. A higher metabolic rate may result in increased energy expenditure and potentially lower weight gain.
Dietary intake: The quantity and quality of the mother’s dietary intake play a significant role in weight gain during pregnancy. Consuming a balanced and nutritious diet supports healthy weight gain.
Vomiting or diarrhea: Frequent vomiting or diarrhea can lead to weight loss or inadequate weight gain during pregnancy. These conditions can affect nutrient absorption and overall caloric intake.
Amount of amniotic fluid: The volume of amniotic fluid surrounding the fetus can contribute to weight gain. An increased amount of amniotic fluid may contribute to higher weight gain.
Size of the fetus: The size and growth rate of the fetus can impact maternal weight gain. A larger fetus may result in increased weight gain during pregnancy.
Maternal physical activity level: The level of physical activity and exercise undertaken by the mother can influence weight gain. Regular physical activity can help maintain a healthy weight during pregnancy.
Maternal genetics: Genetic factors can influence an individual’s predisposition to weight gain or weight retention during pregnancy.
CHANGES IN THE MUSCULO-SKELETAL SYSTEM
Progesterone and Relaxin lead to relaxation of pelvic ligaments, joints and muscles. The relaxation allows the pelvis to increase its capacity in readiness to accommodate the presenting part towards term and also during labour. The symphysis pubis and sacroiliac joints soften, the gait of the mother changes as the balance of the body is altered by the weight of the uterus. Allowing the pelvis to increase its capacity towards term is a process known as a give.
SKIN CHANGES
Increased activity of melanin-stimulating hormone from the pituitary causes varying degrees of pigmentation in pregnant women from the end of 2 nd month until term.The areas that are commonly affected are; areolar of the breasts, abdominal mid line, perineum and axilla. This is because of increased sensitivity of the melanocytes to the hormone or because of greater number of melanocytes in these areas.
- -Linea nigra. This is a dark line that runs from the umbilicus to the symphysis pubis and may extend as high as the sternum. It is hormone induced pigmentation. After delivery, the line begins to fade though it may not ever completely disappear.
- -Mask of pregnancy(Cloasma). This is the brownish hyper pigmentation of the skin over the face, fore head, nose, cheeks and neck. It gives a bronze look especially in black complexioned women.
- -Striae gravidurum(stretch marks).
- -Sweat glands. Activity of the sweat glands usually increases throughout the body which causes the woman to perspire more profusely during pregnancy.
- – A rise in body temperature of 0.5 and increase in blood supply causes vasodilation and makes woman feel hotter.
THANKS it’s simple to understand your work