
Sinciput is the area lying in front of the anterior fontanel and corresponds to the area of brow and the occiput is limited to the occipital bone.
Flat bones of the vault are united together by non-ossified membranes attached to the margins of the bones. These are called sutures and fontanels. Of the many sutures and fontanels, the following are
of obstetric significance.
Bones of the Vault of the Fetal Skull:
The bony structure of the vault originates within a membrane framework. Over time, a process known as ossification hardens these structures from the center outward.
At birth, ossification remains incomplete, resulting in small gaps existing between the bones referred to as sutures and fontanelles. Each bone features a distinct ossification center, which appears as a noticeable protrusion. The full ossification of the skull takes place only in early adulthood.
The vault’s bony composition encompasses:
(i) Two Frontal Bones: Form the forehead (sinciput). Each has an ossification center (frontal eminence). They are square and fuse into a single bone by age 8.
(ii) Two Parietal Bones: Lie on either side of the skull. Each has an ossification center (parietal eminence). They are rectangular.
(iii) Occipital Bone: Lies at the back of the head; part contributes to the skull base, containing the foramen magnum (protecting the spinal cord). It is triangular, with the occipital protuberance as its ossification center.
(iv) Upper segment of the Temporal Bones (both sides): Contribute to the vault(on both sides of the head participates in forming the vault’s structure.)
Development of the Vault:
Five ossification centers develop in the membranes, with calcium deposition (ossification). Chondrocytes contribute to membrane formation. Ossification centers form prominences like frontal bosses, parietal eminences, and the occipital protuberance.
Clinical Notes:
- Premature Infants: Bones are not fully ossified, leaving membranous spaces. This lack of support increases the risk of intracranial injury at birth.
- Full-Term Infants: Narrow areas remain due to incomplete ossification, allowing for molding (overlapping) during labor to facilitate passage through the pelvis.
- Post-Mature Infants: Further ossification leads to harder bones and narrower spaces, hindering molding and making delivery more difficult, with an increased risk of intracranial injury.
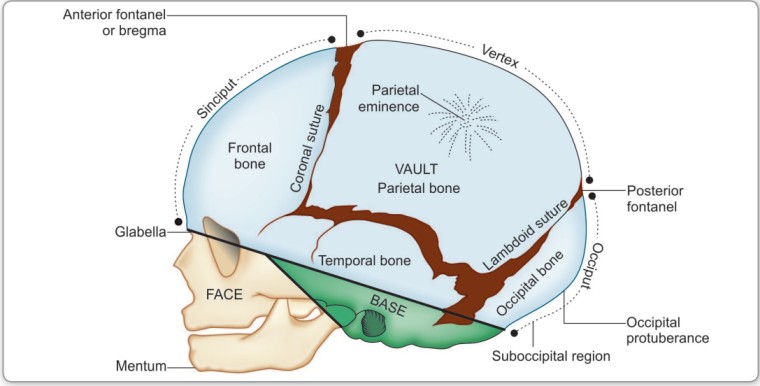
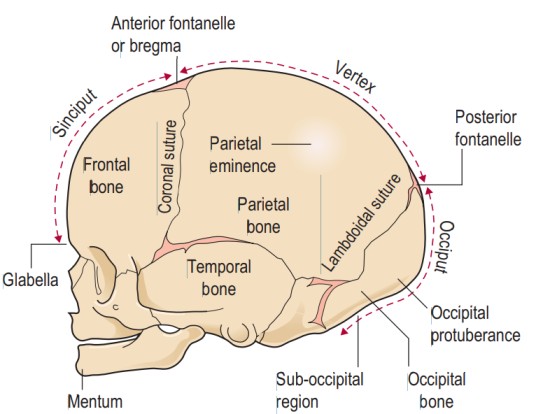 Regions of the Fetal Skull:
Regions of the Fetal Skull:
The fetal skull’s various segments are defined by distinct regions, each marked by significant landmarks(see figure above). These points of reference hold particular importance for midwives during vaginal examinations, aiding in determining the fetal head’s position.
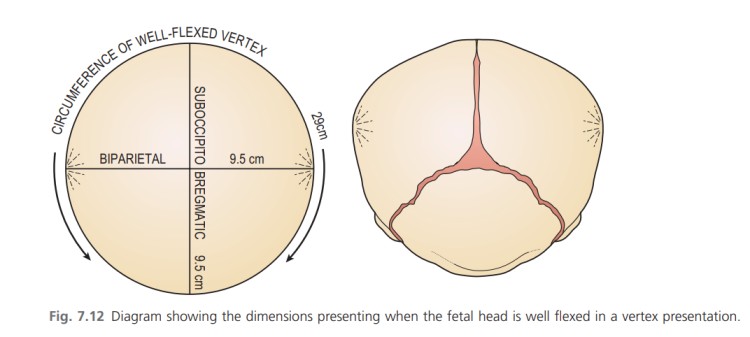
(i) Vertex: The area between the anterior fontanelle (front), posterior fontanelle (behind), and the two parietal eminences (laterally). 95% of babies are present in the vertex position.
(ii) Sinciput (Brow): Extends from the anterior fontanelle and coronal suture to the orbital ridges.
(iii) Face: Extends from the orbital ridges and root of the nose to the chin-neck junction. The chin (mentum) is an important landmark; the face is small in newborns.
• Extending from the orbital ridges and the base of the nose to the junction of the chin, or mentum (landmark), and the neck is the face region. The point situated between the eyebrows is recognized as the glabella
(iv) Occiput: Lies between the foramen magnum and the posterior fontanelle. The area below the occipital protuberance (landmark) is referred to as the sub-occipital region. The protuberance is a prominent point on the skull’s posterior aspect.
SUTURES
Sutures: Membranous lines or cranial joints separating cranial bones. They allow for overlapping during labour.
Important Sutures in Obstetrics:
- Frontal (Metopic) Suture: Between the two frontal bone halves; it obliterates over time.
- Coronal Suture: Separates the frontal and parietal bones.
- Sagittal Suture: Between the two parietal bones.
- Lambdoid Suture: Separates the occipital and parietal bones.
- Squamous Suture: Separates the temporal and parietal bones.
Importance:
- It allows smooth movement of one bone over the other during head molding, which is significant as the head passes through the pelvis during labor.
- Palpating the sagittal suture during internal examination in labor provides insight into head engagement (asynclitism or synclitism), the degree of internal head rotation, and head molding.
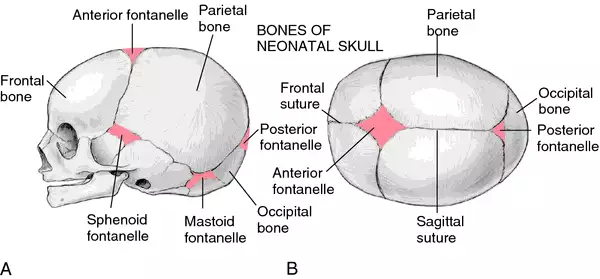
FONTANELS
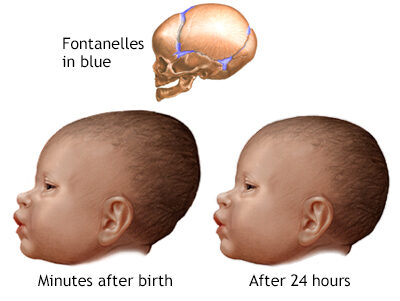
Fontanelles: Membranous spaces where sutures meet; they allow for moulding during labour.
A wide gap in the suture line is referred to as a fontanel. Among the numerous fontanels (total of 6), two hold obstetric significance: (1) Anterior fontanel or bregma and (2) Posterior fontanel or lambda.
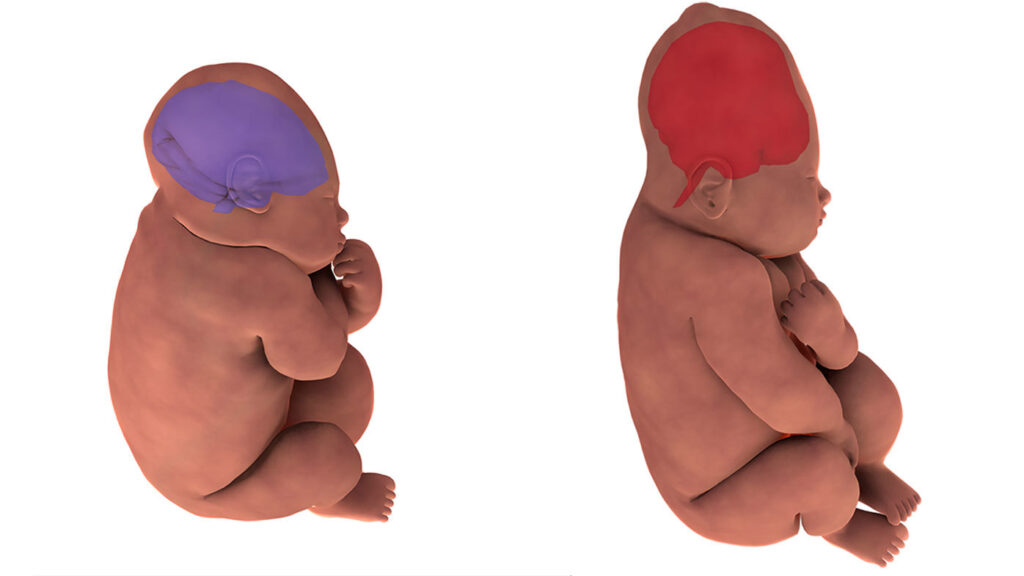
Anterior fontanel: It results from the fusion of four sutures in the midline. The sutures include the frontal suture anteriorly, the sagittal suture posteriorly, and the coronal sutures on either side. Its shape resembles a diamond, with anteroposterior and transverse diameters of approximately 3 cm each. The floor consists of a membrane, which undergoes ossification around 18 months after birth. If ossification does not occur even after 24 months, it becomes pathological.
Importance:
- Palpating it during internal examination indicates the degree of head flexion.
- It aids in head molding.
- Due to its membranous nature persisting after birth, it accommodates significant brain growth, with the brain nearly doubling in size during the first year of life.
- Palpation of the floor reflects intracranial conditions – depressed in dehydration, elevated in raised intracranial pressure.
- In rare cases, blood collection and exchange transfusion can be performed through it, via the superior longitudinal sinus.
- Although uncommon, cerebrospinal fluid can be drawn through the angle of the anterior fontanel from the lateral ventricle.
Posterior fontanel: It is formed by junction of three suture lines — sagittal suture anteriorly and lambdoid suture on either side. It is triangular in shape and measures about 1.2 × 1.2 cm (1/2″ × 1/2″).
Its floor is membranous but becomes bony at term. Thus, truly its nomenclature as fontanel is misnomer.
It denotes the position of the head in relation to maternal pelvis.
Sagittal fontanel: It is inconsistent in its presence. When present, it is situated on the sagittal suture at the junction of anterior two-third and posterior one-third. It has got no clinical importance.
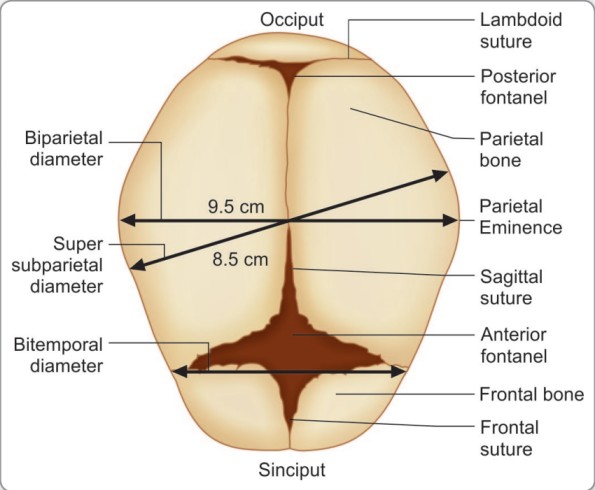
Transverse Diameters
The transverse diameters of the fetal skull;
There are also two transverse diameters,
• The biparietal diameter (9.5 cm) – the diameter between the two parietal eminences.
• The bitemporal diameter (8.2 cm) – the diameter between the two furthest points of the coronal suture at the temples.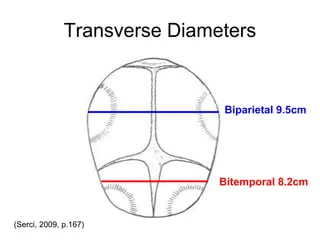
Knowledge of the diameters of the trunk is also important for the birth of the shoulders and breech
- Bisacromial diameter 12 cm: This is the distance between the acromion processes on the two shoulder blades and is the dimension that needs to pass through the maternal pelvis for the shoulders to be born. The articulation of the clavicles on the sternum allows forward movement of the shoulders, which may reduce the diameter slightly.
- Bitrochanteric diameter 10 cm: This is measured between the greater trochanters of the femurs and is the presenting diameter in breech presentation.
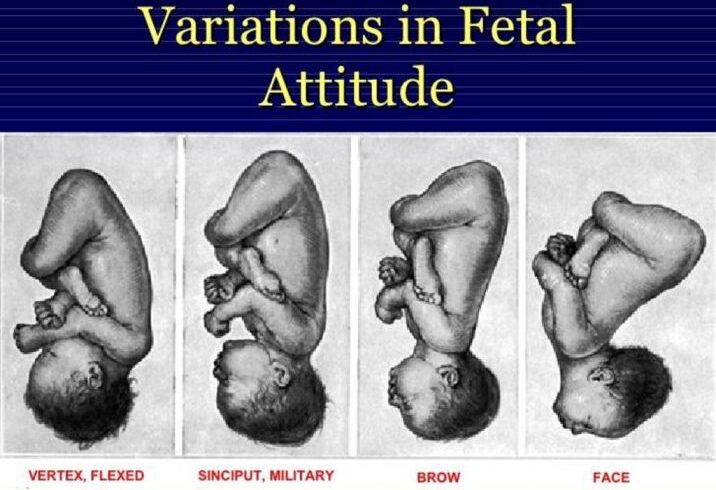
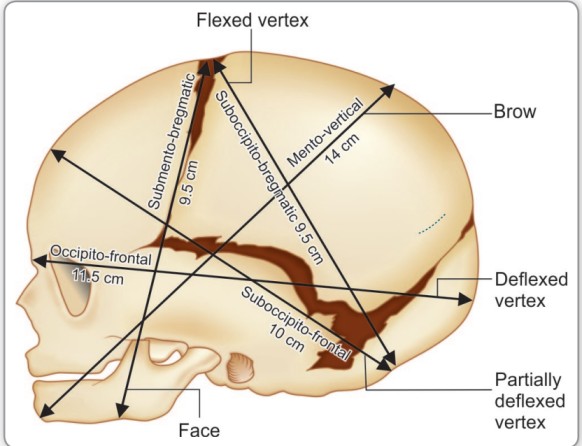
ATTITUDE OF THE FETAL HEAD
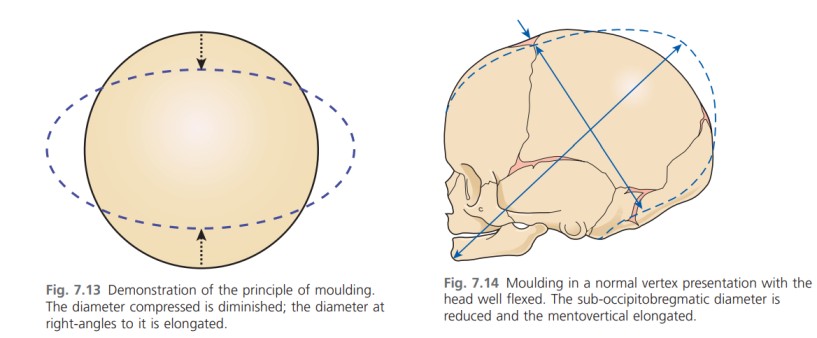
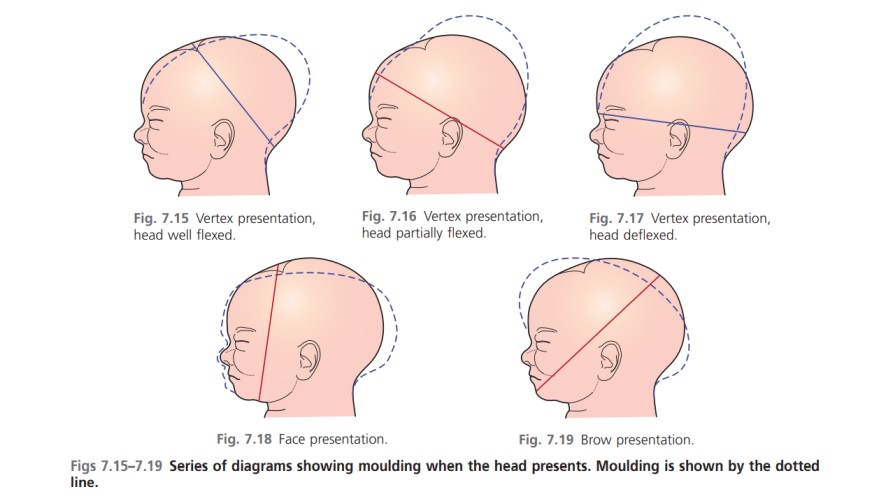
The attitude of the fetal head refers to the degree of flexion or extension of the head relative to the fetal body.
This is a crucial factor influencing which diameter of the fetal skull presents during labor, impacting labor progression and outcome.
A well-flexed head presents smaller diameters, facilitating easier passage through the birth canal.
Conversely, an extended head presents larger diameters, potentially leading to complications.
Presenting Diameters vs. Engaging Diameters:
The terminology used to describe fetal head diameters during labor needs clarification:
- Presenting Diameters: These are the diameters of the fetal skull that are initially oriented at right angles to the curve of Carus (the axis of the birth canal) before the head engages in the pelvis. They are important in determining the initial presentation and lie of the head.
- Engaging Diameters: These are the diameters that present after the head flexes and begins to descend into the pelvic brim. These are the diameters that actively distend the perineum during the second stage of labor. Both longitudinal and transverse diameters are considered engaging diameters.


Thank you for the information
Thank 4enlighting and teaching more and more again 🙏🏾
Good
So interesting and educative
Wauu, this is so precised and easy to understand
Thanks very important notice
wow , thank you!
I love the slides