
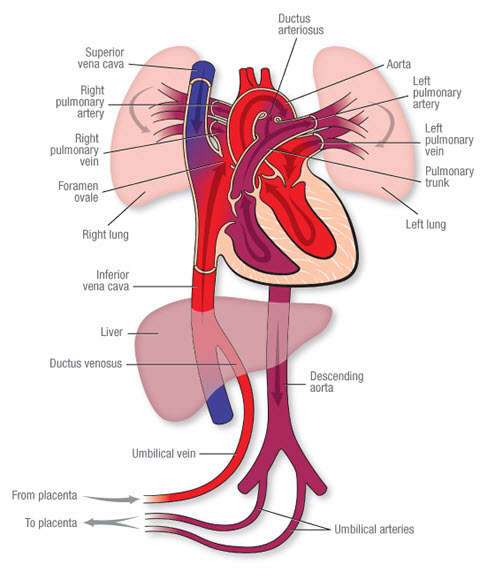
Blood Circulation in Temporary Structures:
(i) Umbilical Vein: Blood from the placenta, 80% saturated with oxygen and nutrients, is transported to the fetus via the umbilical vein. It branches in the liver, joining the portal vein and supplying the liver. This is the only vessel in the fetus carrying unmixed blood.
(ii) Ductus Venosus: Connects the umbilical vein to the inferior vena cava. Here, the blood mixes with partially oxygenated blood returning from the lower body.
(iii) Foramen Ovale: Approximately 75% of the mixed blood passes through this temporary opening between the two atria. This diversion occurs because the blood is already oxygenated and doesn’t need to go to the lungs. A small amount of blood flows through the pulmonary artery to the lungs (to maintain viability) and returns to the left atrium via the pulmonary vein. 25% of this blood enters the left ventricle and then the aorta. The heart and brain receive relatively well-oxygenated blood because the coronary and carotid arteries are early branches. The arms are more developed than the legs at birth because they receive oxygenated blood from the aorta.
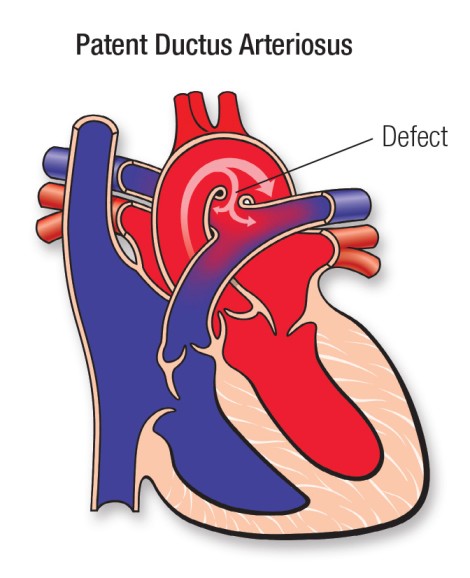
(iv) Ductus Arteriosus: Moves blood from the pulmonary artery to the descending aorta, entering just beyond where the subclavian and carotid arteries branch from the aorta.
(v) Hypogastric Arteries: Blood then flows to the hypogastric arteries (branches of the internal iliac arteries), becoming the umbilical arteries, which return approximately 15% oxygen-saturated blood to the placenta for re-oxygenation.
Simplified Flow:
- Oxygenated blood from the mother enters the placenta.
- Oxygenated blood travels via the umbilical vein to the fetus.
- Most of this blood bypasses the liver via the ductus venosus.
- The blood enters the inferior vena cava.
- Most of the blood flows through the foramen ovale into the left atrium.
- The blood is then pumped to the rest of the body.
- Deoxygenated blood returns to the heart.
- Some blood goes to the lungs, but most is shunted via the ductus arteriosus to the aorta.
- Deoxygenated blood travels back to the placenta through the umbilical arteries.
Mnemonic:
P-U-D-I-F-D-U (sounds like “Poo-dee-fid-you”):
- Placenta: Receives oxygen from mom
- Umbilical Vein: Brings oxygen to baby
- Ductus Venosus: Bypasses liver
- Inferior Vena Cava: Blood mixes
- Foramen Ovale: Bypasses lungs
- Ductus Arteriosus: Bypasses lungs again
- Umbilical Arteries: Returns blood to placenta






1.fetal circulation is the process by which the fetus receives nutrient and oxygen for growth and development during intrauterine life
2.
-umbilical arteries
-ductus venosus
-foramen ovale
-ductus arteriosus
-umbilical veins
3.blood from the mother through the placenta the oxygenated blood is transported by umbilical arteries to supply the liver and in inferior vena cover through ductus venosus it then crosses from the right atrium to the left atrium through foramen ovale then to the left ventricle and pumped to right ventricle to be transported to the upper extremity through aorta which divides in carotid,subclavian ,and returns to the heart then pumped to the lungs for oxygenation through the pulmonary artery via ductus arteriosus blood then will be gassious exchange in the lungs and blood is pumped through the descending aorta which later becomes epigastric arteries then devides I to umbilical vein and back to placenta and the cycle continues
4
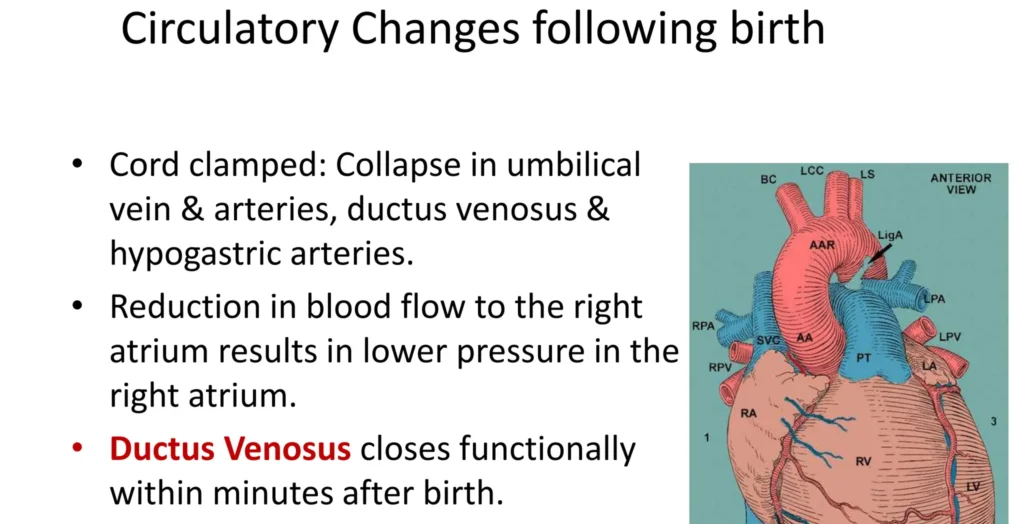
– closure of foramen ovale
– opening of the lungs when the baby cries
–
5.fetal receives from mother while adult is independent
Good lessons
thank you I like your notes
thanks