
Table of Contents
ToggleECTOPIC PREGNANCY
Ectopic pregnancy is a condition in which a fertilized egg implants and grows outside the uterus. Instead of the fertilized egg traveling to and implanting in the uterus as it should during a normal pregnancy, it implants in a location where it cannot develop properly.
Ectopic pregnancy is when the fertilized ovum embeds outside the uterine cavity.
Causes of Ectopic Pregnancy.
Fallopian tube damage: Scarring or blockage in the fallopian tubes, caused by previous infections, surgeries, or conditions like endometriosis, can interfere with the the movement of the fertilized egg through the tube and increase the likelihood of implantation outside the uterus. Congenitally long tubes which are liable to kink, Congenital narrowing of the fallopian tube also increases the risk.
Hormonal factors: Certain hormonal imbalances or abnormalities can affect the movement and implantation of the fertilized egg, increasing the risk of ectopic pregnancy.
Previous ectopic pregnancy: Women who have had an ectopic pregnancy in the past are at a higher risk of experiencing another ectopic pregnancy in the future.
Reproductive system abnormalities: Structural abnormalities of the reproductive system, such as a misshapen uterus or an abnormally located fallopian tube, can contribute to the occurrence of ectopic pregnancy.
Pelvic inflammatory diseases.eg salpingitis. This cause destruction or erosion of Cilia, formation of adhesions interfering with peristalsis in the tubes.
Tumours: pressing on adjacent sides of the tube causing partial or complete blockage of the tube.
Endometriosis ie development of the endometrium in other places other than the uterus.
Repeated induced abortions
Tubal surgery ie surgical procedures on the fallopian tubes may cause intraluminal or extraluminal adhesions.
Intra Uterine Devices. This can interfere with implantation of the fertilized ovum.
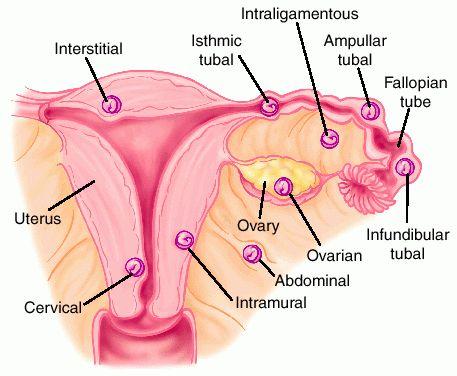
SITES OF ECTOPIC PREGNANCY
The commonest is the uterine tube but can also occur in the broad ligament, ovary and abdominal cavity.
- Fallopian tubes(commonest)
- Ovary
- Intraperitoneal abdominal cavity
- Cervix
Tubal pregnancy
This is when a fertilized ovum embeds it self in the fallopian tubes.
Sites for tubal pregnancy
- Ampulla(commonest)
- Isthmus (e most dangerous because it has tendency to rupture
very early sometimes even before the mother realizes she is pregnant) - Fimbriated end(infundibulum) – rare
- Interstitial part(rare)
POSSIBLE OUTCOMES OF TUBAL PREGNANCY
- Tubal mole: The zygote dies but it is retained in the fallopian tubes surrounded by a blood clot. This may result into a slow leaking ectopic pregnancy
- Tubal abortion: The zygote separates from the fallopian tube lining and it is expelled through the fimbriated end. It may die out or continue to survive on abdominal organs resulting into abdominal pregnancy which can go up to term.
- Tubal rapture: The tube becomes too small for the growing zygote so it raptures causing internal bleeding into the abdominal cavity.
- It is one of the obstetric emergencies since it causes a lot of internal bleeding and thus shock.
- Tubal erosion: The zygote erodes the fallopian tube lining causing bleeding in to the abdominal cavity.
Signs and symptoms ectopic pregnancy (tubal rapture)
On history taking
- History of amenorrhea 6 – 10 weeks
- Patient complains of a feeling of fainting, dizziness, thirsty and vomiting.
- Patient complains of acute abdominal pain localized in the iliac fossa which is colicky in nature. It can be referred to the shoulder especially on lying down due to blood irritating the diaphragmic nerve and peritoneum.
On examination
- Signs of pregnancy are present. eg darkening of areolar.
- Signs of shock i.e. cold, clammy skin, rapid and thread pulse, low blood pressure and temperature.
- Patient is anxious and restless.
- Pallor of the mucous membrane.
On palpation
- Abdominal tenderness especially on the affected side
- Abdominal muscles become rigid due to mother guarding against pain.
- Abdominal distension due to presence of blood in the abdominal cavity
On vaginal examination
- Amount of bleeding doesn’t correspond to the mother’s condition.
- Tenderness on movement of the cervix and a mass is felt in the lateral fornix of the vagina.
- Painful mass in the pouch of Douglas
- Dark brown blood on the examining finger.
Investigations
- Ultra sound scan will reveal the rupture and collection of blood on the affected side. Ultrasound scan will confirm the diagnosis
- Blood for Hb, grouping and cross match.
- On CBC, Haemoglobin level will be low
- Pregnancy test is positive
- In an emergency if scan is not available a puncture into the Pouch of Douglas fresh blood will be found on aspiration
Differential diagnosis
- Salpingitis if associated with irregular menses
- Appendicitis
- Abortion
- Twisted ovarian cyst
- Urinary tract infection
Management of Ectopic Pregnancy
In health centre.
This is an emergency and everything must be done as quickly as possible to save life of the mother.
Aims
- To prevent shock
- To relieve pain
- To reassure the patient
- Admission: Mother is admitted temporarily on gynaecological ward. Histories are taken, general examination, observations, abdominal and vaginal examination done. A diagnosis is then made.
- Histories: these are taken including personal, social, surgical, medical, obstetrical history, how the condition started etc
- Examination: This is carried out from head to toe to rule out anaemia, dehydration, shock etc
- Observation: Temperature, pulse, respiration and blood pressure are taken and recorded to assess functioning of vital organs.
- Resuscitation: A drip of normal saline is put up and morphine 15 mg given intramuscularly. The foot of the bed should be raised to allow blood to move to vital centers.
- Transport: Send for transport as soon as possible and inform the patient and relatives about the decision made and why it is necessary.
- Transfer: The decision is explained to the patient and relatives, a well written note made stating time of admission, treatment given condition on arrival and leaving. Transport is arranged then the mother is transferred to hospital. The midwife escorts the mother and hands her over to the hospital staff.
- Treatment: Put up intravenous infusion of normal saline to prevent or treat shock. This is to elevate the low blood pressure. Administer morphine or pethidine to relieve pain as prescribed.
- Nursing care: The vulva is swabbed and a clean pad is applied. Send the patient to hospital with a written note stating when the patient reported to the center, condition on admission and at time leaving and treatment given.
Hospital Management
In the hospital
It is a gynecological emergency, so everything must be done quickly as possible and all nurses must work as a team to see that the patient is taken for operation as soon as possible.
Aims
- To treat anaemia
- To prevent or treat shock
- To reassure the patient
- To prevent complications
- Admission: Admit the patient in a well-ventilated room and warm admission bed. Establish a good nurse patient relationship.
- Histories :Histories are taken from the patient if able or from the relatives if patient is unable (collateral history).These will include social, medical, surgical, obstetrical, gynaecological histories. More emphasis is put on history of the presenting complaint i.e. when the condition started, amount of bleeding, site of pain, any vomiting or if any treatment has been given. Weeks of amenorrhoea are estimated.
- The doctor is then informed
- General examination: This carried out from head to toe to rule out anemia, shock, dehydration etc
- Observations: Vital observations like temperature, pulse, respiration and blood pressure.
- Investigations: On arrival of the doctor, he orders for the following investigations;
> Haemoglobin estimation to rule out malaria
> Blood group and cross matching because blood transfusion may be necessary
> Pregnancy test to confirm that the mother was pregnant and the pain is not due to other conditions
> Ultra sound scan to confirm the diagnosis
> Urinalysis to rule out urinary tract infection - Resuscitation: Intravenous Normal saline is started to prevent or treat shock. Morphine 15 mg I.M. will be given as ordered by doctor. If mother is in shock it is also managed. Intravenous fluids eg normal saline are put up and fluid balance chart is maintained.
- Blood transfusion: This carried out depending on the haemoglobin results.
- Pain relief: Analgesics such as morphine is administered to relieve pain as prescribed by the doctor.
Pre-operative care
The doctor will determine the operation.
Preparation for theatre
Nursing care
- A bed bath is given, theatre gown offered, observations done and recorded, all charts collected then the patient is wheeled to theatre.
- Explain the nature of operation to the patient and obtain an informed consent.
- Reassure the patient to allay anxiety
- Theatre staffs are informed
- Pass an intravenous line for infusion
- Vulva swabbing is done to minimize infections
- Catheterization is done and a fluid balance chart is started.
- Pass a naso-gastric tube for aspiration gastric or stomach contents or an anti-acid like magnesium trisilicate is given to make the stomach contents alkaline. This prevents aspiration of acidic contents into the lungs.
- Pre- medication is given like atropine to dry the secretions.
- Repeat vital observations and compare with the baseline observations and record.
- Compile the clinical charts and notes, dress the patient in gown and transport her carefully to theatre.
- In theatre give a full report to the theatre nurse about the patient.
- Book about 1-2 units of blood.
- The patient is handed over to the theatre staff and if possible the ward nurse stays with the patient until she is anesthetized. The nurse goes back to the ward and makes a post-operative bed with all its requirements.
In theatre
- Laparatomy and salpingectomy is done to remove the ruptured portion and repair the area to control bleeding. The other tube is examined for patency and unblocked if possible. If the rupture was acute and the blood is fresh it may be collected, sieved into an anticoagulant (sodium citrate) and re-transfused into the patient. This is known as auto transfusion. If this is not possible cross matched blood is transfused.
Post- operative care
- Post-operative bed should be made with all its accessories such as a drip stand, oxygen machine, vital observation tray, emergency tray, resuscitation tray e.t.c. ready to receive the patient.
- When the operation is complete, the ward staff are informed and two qualified nurses go to theatre to collect the patient.
- In theatre, receive a full report from the anesthetic and the theatre nurse in a recovery room should report the condition of the patient.
- Confirm the report while patient is still in the recovery room by;
- Checking airway, breathing and circulation.
- Taking vital observations
- Observing the site of operation for bleeding
- Observe the catheter to see if it is draining well and in good position.
- After confirming, the patient is gently wheeled to ward in a recumbent position with the head turned to one side meanwhile observing the airway.
On ward
- The patient is lifted from the trolley with care to a well made post-operative bed with all its accessories close to the nurse’s station for close observations.
- The patient is put in a recumbent position with the head turned to one side to allow drainage of secretions and also to prevent falling back of the tongue.
Observations and records
- Vital observations of temperature, respiration, blood pressure and pulse are taken1/4 ,1/2, 1, 2 hourly according to surgeon’s instructions and duration is increased as the patient stabilizes.
These observations are continued until the patient is discharged.
- Observe the site of operation for bleeding
- Observe the catheter if it is draining well, colour and the quantity of urine passed.
- Maintain a fluid balance chart and balance it every 24 hours to rule out renal failure.
- On gaining consciousness, the patient is welcomed from theatre, face is sponged, theatre gown changed, mouth wash is done to remove anesthetic smell and a pillow is offered.
Fluid/hydration
- Intravenous fluid.eg 0.9% are continued to replace lost fluids.
- Observation of IV infusion are done such as observing the cannular site for swelling, drip rate and incase of anything it should be corrected.
- Keep monitoring fluid intake and out put to avoid over hydration.
- IV fluids are stopped when bowel sounds are heard and the patient is able to take by mouth.
- Cannula is also removed when necessary.eg if patient has completed intravenous drugs.
Drug therapy
Administer prescribed antibiotics to counteract infections and administer prescribed strong analgesics for pain relief.
- Antibiotics
> Ampicillin 500 mg 6 hourly for 5 days
> Ceftriaxone 2 gm o.d. for 5 days
> Metronidazole 500 mg 8 hourly for 5 days
> Gentamycin 160 mg o.d. for 5 days
Analgesics
> Pethidine 100mg 8 hourly for 3 doses
> Diclofenac 75 mg 8 hourly for 12 hours
> Panadol 1 gm 8 hourly to complete 5 days as soon as patient can take orally. - Monitor the patient for side effects of the drugs given.
- Supportive drugs such as ferrous and folic acid are given to prevent anaemia.
Wound care
- Observe the wound for bleeding and if so add more dressing if soiled change the dressing. Also check signs of infections.
- Carry out daily wound dressing.
- Stitches are removed on the 7th and 8th day alternatingly.
Physiotherapy.
- Encourage the patient to do deep breathing exercise to prevent chest complications like hypostatic pneumonia.
- Also encourage the patient to start with passive exercises such as limb movement then active exercises like walking around to prevent deep vein thrombosis.
Psychotherapy
- In addition to the psychological care given to the patient pre-operatively, she is continuously reassured to allay anxiety.
Diet
- First carryout digestion test and if positive the bowel sounds are heard, start the patient on small sips of water. Soft foods are introduced and given according to the tolerance and should be rich in;
- Proteins to help in tissue repair
- Roughages to prevent constipation
- Carbohydrates for energy
NB: The nasal gastric tube is removed as long as the patient can take orally without any complaint.
Hygiene
- Carryout bed bath on the first day of operation when the patient is still weak and later assist her to the bathroom.
- Carryout mouthcare to prevent neglected mouth complaints like stomatitis, halitosis e.t.c.
- Ensure that the patient’s clothing, bed linen and the surrounding environment are clean.
Bowel and bladder care
- If urine is clear in 24-48 hours, the urethral catheter is removed and patient is encouraged to pass urine.
- The patient is encouraged to pass stool, offered privacy and also given foods rich in roughages to prevent constipation.
- Incase of constipation and conservative measures have failed, give purgatives such as bisacodyl 5-10mg O.D or NOCTE.
Rest and sleep
- The patient is kept in a quiet well-ventilated room, visitors restricted, bright light avoided so as to create a conducive environment for the patient to sleep and rest.
Advice on discharge
When the patient is fit for discharge advise on the following;
- Should have enough rest at home
- Avoid heavy lifting so as to avoid straining the abdominal muscles.
- To come back for review on appointed dates
- To attend ANC clinics when pregnant
- To bring the husband for treatment if the cause of ectopic pregnancy was PIDs.
- To complete the prescribed medications
Complications of ectopic pregnancy
Immediate complications
- Shock
- Peritonitis
- Dehydration
Long term complications
- Sepsis
- Anaemia
- Fibrosis
- Adhesions following surgery
- Recurrence
Thanks it’s very helpful
This is beautiful ❤️