PHYSIOLOGICAL CHANGES IN PREGNANCY
Pregnancy is a remarkable journey where a woman's body undergoes incredible transformations to support a new life. These changes start right after conception and affect almost every part of her body. Understanding these normal changes is crucial for midwives to identify when something might be going wrong.
General Overview
- Purpose: The mother's body adapts to nourish and house the growing baby.
- Timeline: Changes begin early in pregnancy and continue until delivery.
- Importance for Midwives: Knowing what's normal helps midwives recognize signs of potential complications.
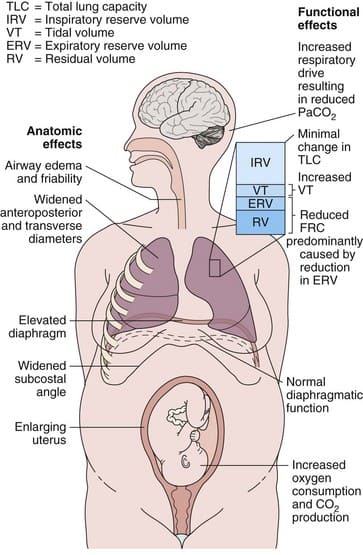
Physical Changes
- Airways: The lining of the airways can become a bit swollen and fragile, making them more sensitive.
- Rib Cage: The rib cage widens and becomes more "barrel-shaped" as the baby grows. This allows more space for the lungs.
- Diaphragm: The diaphragm (the muscle under the lungs) moves up about 4 cm.
- Uterus: The womb (uterus) grows significantly, pushing on other organs.
- Posture: The growing belly changes a woman's center of gravity, often leading to a swayback posture.
- Ligaments: Hormones soften ligaments throughout the body, especially in the pelvis, to prepare for birth.
Breathing Changes (Respiratory System)
- Why the Change? The body needs more oxygen for both the mother and the baby, and it also needs to get rid of more carbon dioxide.
- Breathing Rate: Women often breathe a bit faster and deeper, even at rest.
- Oxygen Use: The body uses about 20% more oxygen during pregnancy.
- Lung Capacity:
- Tidal Volume (amount of air breathed in and out with each normal breath): Increases by about 40%. This means pregnant women take deeper breaths.
- Functional Residual Capacity (FRC - amount of air left in lungs after a normal exhale): Decreases by about 20%. This is because the growing uterus pushes up on the diaphragm, making it harder to fully exhale.
- Overall: While some volumes change, the total amount of air the lungs can hold (Total Lung Capacity) changes only slightly.
- Breathlessness: Many pregnant women feel breathless, even with mild exertion. This is usually normal due to the increased oxygen demand and changes in breathing patterns.
Blood Gas Changes
- Carbon Dioxide (CO2): The level of CO2 in the blood slightly decreases. This is a normal adaptation that helps the baby release its own CO2 into the mother's blood.
- pH: The blood becomes slightly more alkaline (higher pH) due to the lower CO2. This is a compensated respiratory alkalosis.
- Bicarbonate: The kidneys increase the excretion of bicarbonate to help maintain the blood's pH balance.
Important Note for Midwives: If a pregnant woman has a high CO2 level (above 40 mmHg), especially with a fast breathing rate, it could be a sign of respiratory problems.
Cardiovascular Changes (Heart and Blood Vessels)
- Blood Volume: The total amount of blood in the body increases by 30-50%. This helps supply the uterus and placenta and provides a reserve for blood loss during birth.
- Red Blood Cells: While blood volume increases, the plasma (liquid part of blood) increases more than red blood cells, leading to "physiological anemia" or hemodilution. This is a normal finding.
- Heart Rate: The heart beats faster (10-20 beats per minute higher than before pregnancy) to pump the increased blood volume.
- Cardiac Output: The amount of blood pumped by the heart per minute increases significantly (30-50%).
- Blood Pressure: Blood pressure usually drops slightly in the second trimester, then returns to pre-pregnancy levels by the third trimester.
- Swelling (Edema): Increased blood volume and pressure on blood vessels can lead to swelling in the feet, ankles, and hands.
- Varicose Veins/Hemorrhoids: Pressure from the uterus can also contribute to varicose veins and hemorrhoids.
Renal Changes (Kidneys and Urinary System)
- Kidney Size: Kidneys can increase slightly in size.
- Blood Flow: Blood flow to the kidneys increases significantly to filter the increased blood volume and waste products from both mother and baby.
- Urine Production: The kidneys produce more urine, leading to more frequent urination.
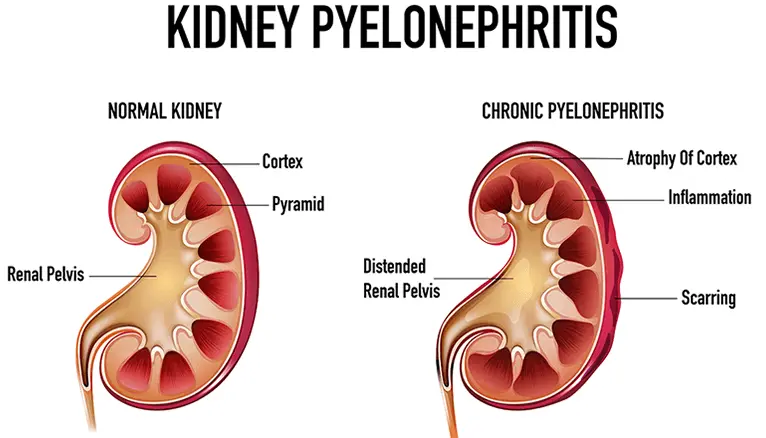
- Bladder: The growing uterus puts pressure on the bladder, also contributing to frequent urination and an increased risk of urinary tract infections.
- Dilated Ureters: The tubes connecting the kidneys to the bladder (ureters) can become dilated, which can sometimes lead to urine reflux and a higher risk of kidney infections.
Gastrointestinal Changes (Digestive System)
- Nausea and Vomiting (Morning Sickness): Very common, especially in the first trimester, due to hormonal changes.
- Heartburn: The growing uterus pushes on the stomach, and hormones relax the sphincter between the esophagus and stomach, allowing stomach acid to reflux.
- Constipation: Hormones slow down the movement of food through the digestive tract, and the uterus can put pressure on the intestines.
- Gallbladder: The gallbladder can become sluggish, increasing the risk of gallstones.
Endocrine Changes (Hormonal System)
Key Hormones: Pregnancy is driven by a symphony of hormones, primarily:
| hCG (human chorionic gonadotropin) | Maintains the corpus luteum in early pregnancy, detected in pregnancy tests. |
| Estrogen | Promotes uterine growth, breast development, and increases blood flow. |
| Progesterone | Maintains the uterine lining, relaxes smooth muscles (contributing to constipation and heartburn), and prevents premature contractions. |
| Relaxin | Softens ligaments and cartilage, especially in the pelvis. |
| Prolactin | Prepares breasts for milk production. |
| Oxytocin | Involved in contractions during labor and milk ejection. |
- Thyroid Gland: The thyroid gland often enlarges slightly and becomes more active.
- Pancreas: The pancreas works harder to produce insulin to manage blood sugar, as pregnancy can create some insulin resistance.
Musculoskeletal Changes
- Joint Loosening: Hormones like relaxin loosen joints and ligaments, especially in the pelvis, to prepare for birth. This can lead to back pain and pelvic discomfort.
- Center of Gravity: The growing uterus shifts the woman's center of gravity forward, leading to changes in posture and balance.
- Diastasis Recti: The abdominal muscles can separate (diastasis recti) as the uterus expands.
Skin and Hair Changes
- Hyperpigmentation: Darkening of the skin can occur, especially on the face (melasma or "mask of pregnancy") and a dark line down the abdomen (linea nigra).
- Striae Gravidarum (Stretch Marks): Pink or purple lines can appear on the abdomen, breasts, and thighs as the skin stretches.
- Hair Growth: Many women notice thicker hair during pregnancy, but some may experience hair loss after delivery.
- Vascular Spiders/Palmar Erythema: Small, red spider-like blood vessels (vascular spiders) and redness on the palms (palmar erythema) are common due to increased estrogen.
ASTHMA IN PREGNANCY
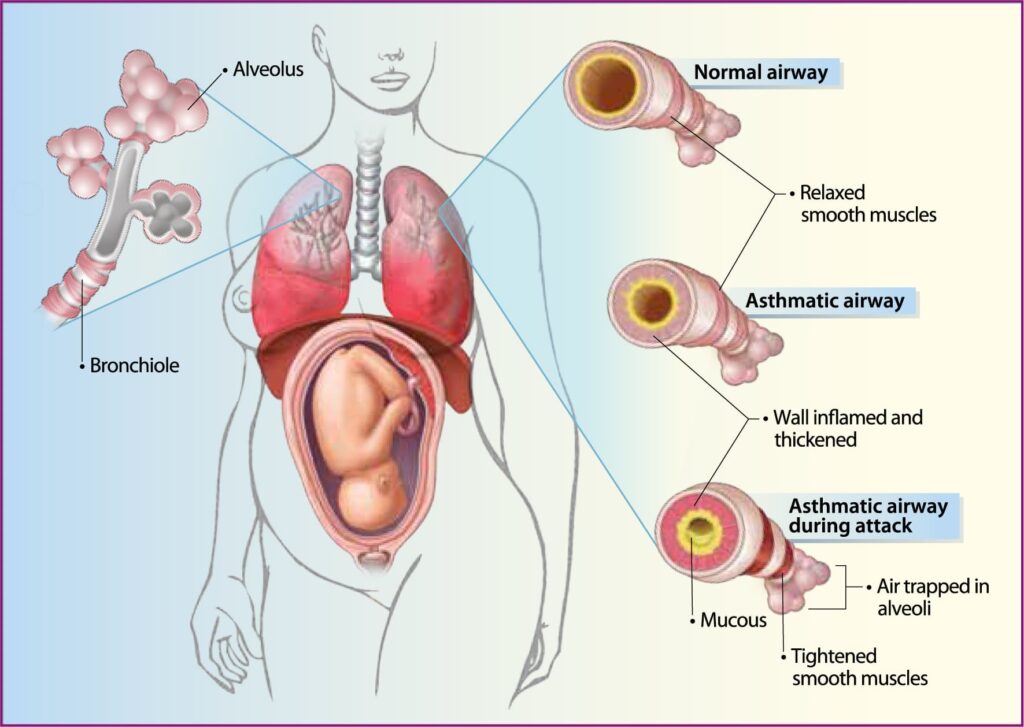
Asthma is a common and chronic lung condition that causes inflammation and narrowing of the airways, leading to breathing difficulties. When a pregnant woman has asthma, careful management is essential to ensure the health of both mother and baby.
What is Asthma?
Asthma is like a "twitchy" airway disease. When triggered, the airways in the lungs become inflamed, swell, and produce extra mucus. The muscles around the airways also tighten (bronchoconstriction), making it hard to breathe. These changes are usually reversible with treatment.
- Common: Asthma is one of the most common chronic conditions in pregnant women.
- Impact on Mother: Poorly controlled asthma can lead to severe asthma attacks, hospitalization, and even death.
- Impact on Baby: Severe asthma attacks in the mother, especially those causing low oxygen levels (hypoxemia), can harm the baby. This is because the baby relies on the mother for oxygen.
Risk Factors for Developing Asthma
These factors don't just apply to pregnant women, but they can influence the severity of asthma:
- Genetics: Having parents with asthma or allergies increases the risk.
- Environmental Triggers:
- Allergens: Dust mites, pollen, pet dander, mold.
- Irritants: Tobacco smoke (active or passive), air pollution, strong fumes (e.g., cleaning products).
- Lifestyle:
- Obesity: Maternal obesity can increase the risk of more severe asthma.
- Diet: A "Western diet" (high in processed foods) may be linked to higher asthma risk.
- Early Life Factors: Antibiotic use, infections, and reduced sun exposure in childhood may play a role.
- Other Conditions: Stress, depression, and violence can worsen asthma symptoms.
Pathophysiology of Asthma
Imagine your immune system as a security guard. In asthma, this guard sometimes overreacts to harmless substances (allergens).
- First Contact: When an allergen (like dust mite) enters the airways, specialized immune cells "present" it to other immune cells called T-lymphocytes.
- Overreaction: In asthma, these T-lymphocytes often develop into a specific type (Th-2 cells).
- Chemical Messengers (Cytokines): These Th-2 cells release chemical messengers (cytokines like IL-4, IL-5, IL-9, IL-13) that act like alarm signals.
- Inflammatory Cells Activated: These signals recruit and activate other immune cells like mast cells, basophils, and eosinophils. These cells are particularly involved in allergic reactions.
- Histamine & More: These activated cells then release powerful inflammatory chemicals (like histamine, prostaglandins, and leukotrienes).
- Airway Response: These chemicals cause:
- Bronchial hyperresponsiveness: The airways become extra sensitive and easily constrict.
- Airway obstruction: The airways narrow, making it hard to breathe.
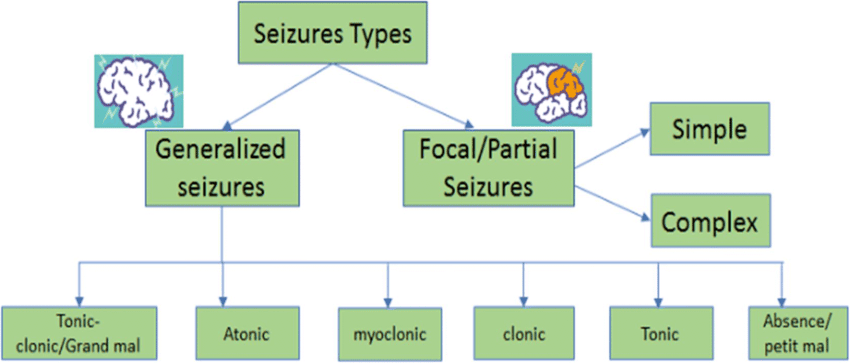
Symptoms & Warning Signs
Symptoms (What you might experience):
- Chest tightness: Feeling like a band is squeezing your chest.
- Coughing: Often worse at night, with exercise, or when laughing.
- Difficulty breathing/Shortness of breath: Feeling like you can't get enough air.
- Wheezing: A whistling sound, especially when breathing out.
- Sleep problems: Waking up due to coughing or breathlessness.
Warning Signs (Early indicators that your asthma might be getting worse):
- Headache, stuffy or runny nose, sore throat (could indicate a cold triggering asthma).
- Coughing or wheezing after exercise.
- Trouble sleeping.
- Feeling moody or irritable.
- Feeling unusually tired or weak during physical activity.
How is Asthma Diagnosed?
Diagnosis often involves looking at your symptoms and measuring your lung function.
- Peak Expiratory Flow Rate (PEFR) or Forced Expiratory Volume in one second (FEV1): These are common lung function tests.
- PEFR: Measures how fast you can exhale air.
- FEV1: Measures how much air you can force out in one second.
- Diagnostic Criteria (in non-pregnant individuals, but principles apply):
- Significant daily variations in PEFR readings over several days.
- Improvement in FEV1 by 15% or more after using a bronchodilator (medication that opens airways) or a course of steroids.
- A significant drop in FEV1 after exercise.
- Chest X-Ray (rarely needed for diagnosis, but may show signs in severe cases):
- Lungs that look "hyperinflated" (too much air trapped).
- Flattened diaphragm.
- Ribs that appear more horizontal.
How Does Pregnancy Affect Asthma?
The good news is that with proper management, most pregnant women with asthma have healthy pregnancies. However, poorly controlled asthma can lead to complications:
- For the Mother: Increased risk of severe asthma attacks.
- For the Baby:
- Pre-eclampsia: A serious condition involving high blood pressure during pregnancy.
- Intrauterine Growth Restriction (IUGR): The baby doesn't grow as expected in the womb.
- Preterm birth: Baby born before 37 weeks of pregnancy.
- Low birth weight: Baby born weighing less than 5.5 pounds.
The main concern: When asthma is severe and poorly controlled, the mother's oxygen levels can drop (hypoxemia). This directly reduces oxygen supply to the baby, leading to these complications.
A DANGEROUS MISCONCEPTION: Many women stop their asthma medications during pregnancy because they worry about safety for the baby. This is extremely dangerous! The risks of uncontrolled asthma to both mother and baby are far greater than the risks of well-established asthma medications.
How Does Pregnancy Affect Asthma? (The "Rule of Thirds")
It's unpredictable how pregnancy will impact a woman's asthma:
- 1/3 of the time: Symptoms get worse.
- 1/3 of the time: Symptoms stay the same.
- 1/3 of the time: Symptoms improve.
During Labor and Postpartum:
- Labor: Acute asthma attacks are uncommon during labor because the body naturally produces steroids that help prevent them.
- Immediately Postpartum: The risk of an asthma flare-up is higher in the period immediately after birth.
- Long-term: Asthma severity usually returns to its pre-pregnancy level within a few weeks or months after delivery.
Managing Asthma in Pregnancy: Goals and Interventions
The main goal: To maintain optimal asthma control throughout pregnancy, ensuring good oxygenation for both mother and baby, while minimizing medication side effects.
General Principles:
- Optimize Before Pregnancy: Ideally, a woman's asthma should be well-controlled before she becomes pregnant.
- Regular Monitoring: Close monitoring of lung function (e.g., home peak flow monitoring) and symptoms.
- Avoid Triggers: Identify and avoid personal asthma triggers (e.g., allergens, smoke).
- Smoking Cessation: Absolutely crucial to stop smoking (including passive smoking).
Interventions
- Individualized Asthma Action Plan: Develop a written plan with the patient, outlining daily management, what to do when symptoms worsen, and when to seek emergency care. This is critical for patient empowerment.
- Proper Inhaler Technique: Regularly check and re-teach correct inhaler technique to ensure medication reaches the lungs effectively. Many patients use inhalers incorrectly.
- Peak Flow Monitoring: Encourage daily home peak flow monitoring. Teach the woman how to interpret her readings and when to adjust medication or seek medical advice based on her personal best.
- Regular Medical Review: Schedule frequent visits with the healthcare team (GP, midwife, asthma specialist) to assess asthma control, review medications, and address any concerns.
-
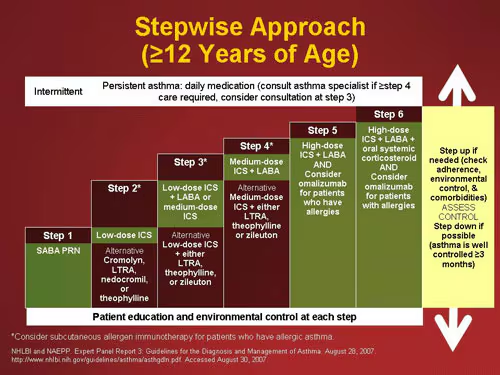
Pharmacotherapy (Medication Management - Stepwise Approach):
- General Rule: Continue all necessary asthma medications during pregnancy. The benefits of controlled asthma far outweigh the theoretical risks of most commonly used asthma medications.
- Most Medications are Safe: Inhaled corticosteroids (ICS) and beta-2 agonists are generally considered safe and the preferred treatments. Oral steroids may be used for severe exacerbations under medical supervision.
Step Level Protocol Step 1
(Mild Intermittent)Inhaled short-acting beta-2 agonist (SABA, e.g., salbutamol) as needed for quick relief of symptoms. Step 2
(Regular Preventer)Add a low-dose inhaled corticosteroid (ICS, e.g., beclomethasone, budesonide) at 200-800 mcg/day. This is the cornerstone of prevention. Step 3
(Add-on Therapy)If asthma is still not controlled, add a long-acting beta-2 agonist (LABA, e.g., formoterol, salmeterol) to the ICS. Continue the ICS. - If there is a good response, continue the LABA.
- If there is some benefit but still inadequate control, continue LABA and increase inhaled steroid dose up to 800 mcg/day.
- If there is no response to LABA, stop LABA and increase inhaled steroid dose (e.g., to 800 mcg/day or higher within the guidelines of Step 4).
- Important: LABAs should never be used alone without an ICS in asthma.
Step 4
(Persistent Poor Control)Consider increasing the inhaled steroid dose up to 2000 mcg/day, and/or adding a fourth drug like a leukotriene receptor antagonist (LTRA, e.g., montelukast) or sustained-release theophylline (less common in pregnancy). Referral to an asthma specialist is essential at this stage. Step 5
(Severe Asthma)For severe, uncontrolled asthma, daily oral steroid tablets (at the lowest effective dose) may be necessary, while maintaining a high dose of inhaled steroid. This requires close specialist supervision and referral to an asthma specialist. - Education on Medication Safety: Reassure patients about the safety of their asthma medications during pregnancy. Provide evidence-based information to counter misinformation. Emphasize that uncontrolled asthma is a greater risk.
- Environmental Control: Advise on measures to reduce exposure to allergens and irritants at home and work (e.g., mattress covers, regular cleaning, avoiding strong scents, ensuring good ventilation).
- Flu and Pneumococcal Vaccinations: Recommend annual influenza vaccination and pneumococcal vaccination (if indicated) to prevent respiratory infections that can trigger asthma attacks.
- Management of Comorbidities: Address co-existing conditions that can worsen asthma, such as rhinitis, sinusitis, gastroesophageal reflux disease (GERD), and obesity.
- Nutritional Counseling: Ensure adequate vitamin D intake, as low vitamin D levels have been linked to asthma severity.
- Stress Management: Provide strategies for managing stress, as stress can be an asthma trigger. Refer for counseling if needed.
- Labor and Delivery Plan: Develop a plan for asthma management during labor and delivery, including what medications to have available. Reassure that labor generally does not trigger asthma attacks.
- Postpartum Follow-up: Schedule a postpartum review to assess asthma control, adjust medications if needed, and discuss future pregnancy planning.
- Breastfeeding Guidance: Reassure mothers that most asthma medications are safe to continue while breastfeeding.
TUBERCULOSIS (TB) IN PREGNANCY
Tuberculosis (TB), caused by the bacterium Mycobacterium tuberculosis, is a serious infectious disease. When it occurs during pregnancy, it requires careful and immediate management to protect both the mother and her unborn child.
Overview & Importance
- The Cause: TB is caused by the bacterium Mycobacterium tuberculosis, which typically forms characteristic "caseating granulomas" (a type of inflamed tissue) in the body.
- Global Health Challenge: The number of TB cases is increasing worldwide, largely due to factors like HIV susceptibility, which weakens the immune system.
- Pregnancy's Role: Pregnancy itself does not increase the risk of getting TB, nor does it change how the disease progresses or spreads.
- The Danger of Untreated TB: If active TB is left untreated during pregnancy, it carries a very high mortality rate (30-40%) for both the mother and her baby.
- Key Message: Early diagnosis and prompt treatment are vital!
Clinical Presentation of Tuberculosis
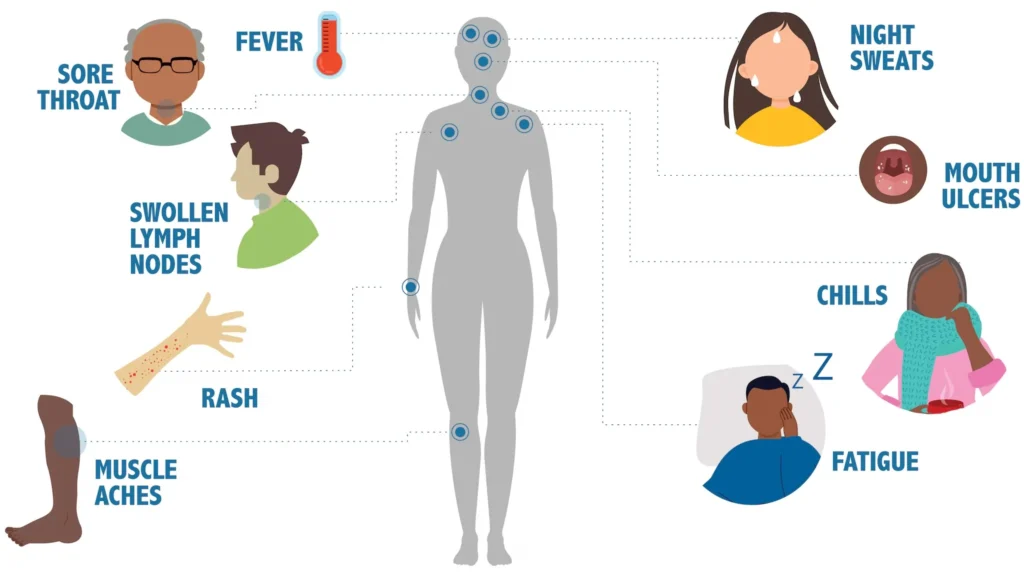
TB can sometimes be "silent," meaning the patient has no symptoms. However, common symptoms include:
- General: Fever, night sweats, unexplained weight loss.
- Respiratory (Lung TB): A persistent cough (lasting more than 2-3 weeks), coughing up blood (hemoptysis), chest pain, and shortness of breath.
- Extra-Pulmonary TB: A significant proportion (up to 50%) of TB in pregnancy can affect areas outside the lungs, such as lymph nodes, bones, liver, or spleen. This is often harder to diagnose.
Diagnosing TB in Pregnancy
- Screening (Mantoux Test / TST): This skin test checks for previous exposure to TB.
- Negative Result: No further action unless the patient is symptomatic or at high risk.
- Positive Result: Indicates exposure, but not necessarily active disease. Requires further investigation.
- Confirmation of Active TB:
- Chest X-Ray: This is often the first step if the Mantoux test is positive or if symptoms suggest lung TB. It's done with proper abdominal shielding to protect the baby. X-ray patterns might show:
- Enlarged lymph nodes (lymphadenopathy).
- Infiltrates (shadows indicating inflammation or infection).
- Sputum Examination: The gold standard for confirming lung TB.
- Acid-Fast Bacilli (AFB) Smear: Sputum is stained (Ziehl-Neelsen stain) and examined under a microscope to look for the TB bacteria.
- Culture: Sputum is cultured to grow the bacteria, which allows for definitive identification and drug sensitivity testing.
- Rapid Molecular Tests:
- GeneXpert / CBNAAT (Cartridge-Based Nucleic Acid Amplification Test): These tests are highly sensitive and can detect M. tuberculosis DNA and resistance to Rifampicin (a key TB drug) within hours.
- Chest X-Ray: This is often the first step if the Mantoux test is positive or if symptoms suggest lung TB. It's done with proper abdominal shielding to protect the baby. X-ray patterns might show:
General Management Principles
- Ideal Scenario: Ideally, women with active TB should complete their treatment before becoming pregnant.
- Active TB in Pregnancy: If active TB is diagnosed during pregnancy, treatment must NOT be delayed. The risks of untreated TB far outweigh the potential risks of the medications.
- Drug Safety (Crucial for Pregnancy):
- Generally Safe (Categories B/C): Rifampicin, Isoniazid (INH), Pyrazinamide, and Ethambutol are generally considered safe and are the first-line drugs for TB.
- ABSOLUTELY CONTRAINDICATED (Category D): Streptomycin is strictly avoided in pregnancy because it causes permanent damage to the baby's 8th cranial nerve, leading to hearing loss (ototoxicity).
- Nutritional Support: Continue all essential supplements: Iron, Folic Acid, Calcium, and other vitamins. This is vital for both mother and baby, especially during TB treatment.
Standard Treatment Regimens
These are general guidelines; specific regimens may vary based on national protocols and individual patient factors. Treatment typically involves an initial intensive phase followed by a continuation phase.
| Category | Patients | Regimen Initial Phase (IP) | Regimen Continuation Phase (CP) |
|---|---|---|---|
| Category I | New smear-positive pulmonary TB, New smear-negative pulmonary TB with extensive lung involvement, Severe concomitant HIV, Severe extra-pulmonary TB | 2 HRZE (2 months of Isoniazid, Rifampicin, Pyrazinamide, Ethambutol) | 4 HR (4 months of Isoniazid, Rifampicin) |
| Category II | Previously treated sputum-positive cases (e.g., relapse, treatment after default, treatment failure) | 2 HRZES / 1 HRZE (2 months of 5 drugs + 1 month of 4 drugs, with 'S' indicating Streptomycin) Note: For pregnant women, Streptomycin (S) is NEVER used. The regimen would be modified (e.g., 2 HRZE / 1 HRZE, omitting S). |
5 HRE (5 months of Isoniazid, Rifampicin, Ethambutol) |
| Category III | New smear-negative pulmonary TB, Less severe extra-pulmonary TB | 2 HRZ (2 months of Isoniazid, Rifampicin, Pyrazinamide) | 4 HR (4 months of Isoniazid, Rifampicin) |
| Category IV | Chronic & MDR-TB cases (Multi-Drug Resistant TB) | Highly specialized regimen, often involving 5-6 drugs for an extended period. | Example for MDR: Kanamycin, Ofloxacin, Ethionamide, Pyrazinamide, Ethambutol, Cycloserine for 6-9 months. Then Ofloxacin, Ethionamide, Ethambutol, Cycloserine for 18 months. |
Drug Specifics & Side Effects
| Drug | Dose & Side Effects | Pregnancy Intervention |
|---|---|---|
| Isoniazid (INH) |
Dose: 5 mg/kg/day. Side Effects: Hepatitis, Peripheral neuropathy (nerve damage). |
Always give with Pyridoxine (Vitamin B6), typically 10-50 mg/day, to prevent peripheral neuropathy in both mother and baby. |
| Rifampicin |
Dose: 10 mg/kg/day. Side Effects: Hepatitis, turns urine/tears orange. |
Give Vitamin K (10 mg orally) to the mother from 36 weeks of gestation until delivery, and to the neonate at birth, to prevent hemorrhagic disease of the newborn. |
| Ethambutol |
Dose: 15-25 mg/kg/day. Side Effects: Retrobulbar neuritis (inflammation of the optic nerve, can cause vision changes). |
Monitor vision monthly. Perform baseline and monthly eye exams (visual acuity, color vision) to detect early changes. |
| Pyrazinamide |
Dose: 15-30 mg/kg/day. Side Effects: Hepatotoxicity (liver damage). |
Monitor liver function tests (LFTs) regularly. |
| Streptomycin | ABSOLUTELY AVOIDED due to fetal ototoxicity. | |
Managing Multi-Drug Resistant TB (MDR-TB) in Pregnancy
This is a complex situation requiring specialized management.
Critical Warning: Second-line injectable drugs commonly used for MDR-TB (Amikacin, Kanamycin, Capreomycin) are CONTRAINDICATED in pregnancy due to their ototoxicity (harm to the baby's hearing).
Ethionamide: Another MDR-TB drug, Ethionamide, is contraindicated in the first 32 weeks of pregnancy due to its potential for causing birth defects (teratogenicity).
Modified Protocol for MDR-TB in Pregnancy:
- Before 20 Weeks of Gestation:
- Option 1: Medical Termination of Pregnancy (MTP): This should be discussed with the patient, especially if the regimen cannot be adequately modified to be safe, or if severe birth defects are a significant concern. The final decision rests with the patient.
- Option 2: Continue Pregnancy with Modified Regimen (if patient unwilling for MTP):
- <= 12 weeks: Omit Kanamycin and Ethionamide. Add Para-aminosalicylic acid (PAS, which is generally safer).
- > 12 weeks (but < 20 weeks): Omit Kanamycin only. Add PAS.
- Post-Delivery: Replace PAS with Kanamycin once the baby is born.
- After 20 Weeks of Gestation:
- Start a modified Category IV regimen (MDR-TB regimen).
- Omit Kanamycin. Add PAS until delivery.
Neonatal Care & Breastfeeding
- Congenital TB: TB infection passed from mother to baby during pregnancy or birth is rare.
- Diagnosis: Often indicated by primary hepatic granulomas in the baby or diagnosis within days of birth.
- Mortality: Even with treatment, congenital TB has a high mortality rate (22%).
- Breastfeeding: Strongly Encouraged! The amount of anti-TB drugs excreted into breast milk is very low and generally safe for the baby.
- If the mother is on Isoniazid, the infant should be monitored.
- Infant Management (Interventions):
- Screen for Active TB: All babies born to mothers with TB should be thoroughly screened for signs of active TB disease.
- Isoniazid Prophylaxis (IPT): If the mother has active, sputum-positive TB, the neonate should receive prophylactic Isoniazid (IPT) to prevent them from developing TB.
- BCG Vaccination: Once active TB has been ruled out and/or the course of IPT is completed, the baby should receive the BCG vaccine as soon as possible.
- Isolation: The mother and baby only need to be isolated if the mother has sputum-positive TB and has been on effective treatment for less than 10-14 days (or is not yet sputum negative). Once the mother is no longer infectious, isolation is not required.
Additional Interventions for Holistic Care
- Patient Education and Counseling: Provide clear, empathetic information about TB, its treatment, the importance of adherence, potential side effects, and reassurance about safety in pregnancy and breastfeeding.
- Multidisciplinary Team Approach: Involve obstetricians, pulmonologists/infectious disease specialists, pediatricians, dietitians, and social workers to ensure comprehensive care.
- Directly Observed Treatment (DOT): For all TB patients, especially pregnant women, implementing DOT ensures medication adherence, which is critical for treatment success and preventing drug resistance.
- Regular Monitoring of Adherence and Side Effects: Beyond specific drug monitoring (e.g., LFTs, vision), regularly check if the patient is taking her medications as prescribed and experiencing any new or worsening side effects.
- Psychosocial Support: Pregnancy is already a vulnerable time. A TB diagnosis can add significant stress. Provide access to counseling, support groups, and address any social or economic barriers to care.
- Contact Tracing: Identify and screen all close contacts of the pregnant woman to prevent further spread of TB.
- Follow-up Post-Delivery: Ensure continuous follow-up for the mother to complete her TB treatment and for the baby to monitor for TB development and developmental milestones.
- HIV Co-infection Management: If the pregnant woman also has HIV, manage both conditions concurrently, as HIV significantly impacts TB progression and treatment.
PNEUMONIA IN PREGNANCY
Pneumonia, an infection that inflames the air sacs in one or both lungs, can be particularly serious during pregnancy. Prompt recognition, diagnosis, and aggressive management are essential to safeguard both the mother and the fetus.
Overview & Significance
- Incidence: Pneumonia is not uncommon in pregnancy, affecting approximately 0.8 to 2.7 out of every 1000 deliveries.
- Severity: A significant concern is the risk of respiratory failure, which occurs in about 10% of pregnant women with pneumonia. This can be life-threatening for both mother and baby.
- Why Pregnancy is Different:
- Physiological Changes: Pregnancy causes natural changes in the respiratory system (e.g., elevated diaphragm, increased oxygen demand) that can make pregnant women more susceptible to severe pneumonia and compromise their ability to cope with lung infection.
- Immunosuppression: The maternal immune system is naturally modulated during pregnancy, which can increase susceptibility to certain infections.
- Key Message: Pneumonia in pregnancy is a serious condition requiring urgent medical attention.
Risk Factors of Pneumonia
Certain conditions or factors can make a pregnant woman more vulnerable to developing pneumonia or experiencing a more severe course:
- Weakened Immune System:
- HIV: Significantly increases the risk, particularly for opportunistic infections.
- Underlying Lung Conditions:
- Asthma: Chronic inflammation of airways makes lungs more susceptible.
- Cystic Fibrosis: A genetic disorder causing thick mucus buildup in the lungs.
- Medications:
- Tocolytic Therapy: Drugs used to stop premature labor (e.g., terbutaline, magnesium sulfate) can sometimes lead to pulmonary edema, which increases susceptibility to pneumonia.
- Corticosteroid Therapy: Used for various conditions (e.g., fetal lung maturation, asthma exacerbations) can suppress the immune system.
- Other Health Issues:
- Anemia: Reduced oxygen-carrying capacity can worsen outcomes.
- Malnutrition: Compromises overall immune function.
- Diabetes: Impairs immune response.
- Heart Disease: Can exacerbate respiratory distress.
- Lifestyle Factors:
- Smoking/Drug Abuse: Damages lung tissue and impairs immune function.
- Exposure to Environmental Pollutants: Increases lung irritation.
Clinical Features of Pneumonia
The symptoms of pneumonia in pregnancy are similar to those in non-pregnant individuals but may be more pronounced.
- Classic Signs:
- Abrupt onset of fever with chills.
- Productive cough: Coughing up mucus or phlegm.
- Tachypnea: Rapid breathing (respiratory rate > 20 breaths/min).
- Tachycardia: Rapid heart rate (maternal heart rate > 100 beats/min).
- Other Symptoms:
- Chest pain (often sharp, worse with breathing).
- Shortness of breath (dyspnea).
- Generalized fatigue, muscle aches.
- Loss of appetite.
- Physical Examination Findings:
- Localized Harsh Sounds: On lung auscultation (listening with a stethoscope), crackles, rhonchi, or bronchial breath sounds may be heard over affected areas.
- Dullness to Percussion: Over areas of consolidation.
- Specific Pathogens to Consider:
- Varicella (Chickenpox) and Influenza (Flu) Pneumonia: These viral pneumonias can be exceptionally severe and often fatal during pregnancy. Early recognition and treatment are critical.
- Pneumocystis jirovecii Pneumonia (PCP): Patients with HIV are highly susceptible to this opportunistic fungal pneumonia.
Diagnosis of Pneumonia
Diagnosis relies on a combination of clinical suspicion, imaging, and laboratory tests.
- Chest X-Ray: This is the cornerstone of diagnosis.
- Safety: Always perform with abdominal shielding to minimize fetal radiation exposure. The risk to the fetus from a single diagnostic chest X-ray is considered negligible compared to the risk of untreated pneumonia.
- Findings: Typically shows consolidation (whitening) in one or more lung lobes.
- Laboratory Tests:
- Sputum and Blood Cultures: Collect these BEFORE administering antibiotics to identify the causative organism and guide targeted therapy.
- Sputum Gram Stain: Rapidly identifies common bacterial types.
- Blood Cultures: Can detect bacteremia (bacteria in the bloodstream), indicating a more severe infection.
- Complete Blood Count (CBC): Often shows leukocytosis (elevated white blood cell count).
- Renal and Liver Function Tests: To assess overall organ function and guide drug dosing.
- C-Reactive Protein (CRP) / Procalcitonin: Inflammatory markers that can help assess severity and response to treatment.
- Arterial Blood Gas (ABG): For moderate to severe cases, to assess oxygenation and acid-base status.
- HIV Test: Consider for at-risk individuals or those with severe, atypical pneumonia.
- Influenza/RSV Swabs: Nasopharyngeal swabs for viral testing during flu season.
- Sputum and Blood Cultures: Collect these BEFORE administering antibiotics to identify the causative organism and guide targeted therapy.
- Oxygen Saturation Monitoring: Continuously monitor peripheral oxygen saturation (SpO2).
- Target: Maintain SpO2 > 94%. If oxygen saturation drops, supplemental oxygen should be provided immediately.
Assessing Severity: CURB-65 Scoring
The CURB-65 score is a simple clinical prediction rule used to assess the severity of pneumonia and guide decisions about inpatient vs. outpatient management, and the need for ICU admission.
- Confusion (new-onset disorientation to person, place, or time)
- Urea > 7 mmol/L (or BUN > 19 mg/dL)
- Respiratory rate > 30 breaths/minute
- Blood pressure (Systolic < 90 mmHg or Diastolic < 60 mmHg)
- Age > 65 years (Note: This component needs careful interpretation in pregnancy, as young pregnant women can still have severe disease. Focus more on the other parameters in this specific context.)
| Score | Interpretation & Management |
|---|---|
| 0-1 points | Low severity; typically suitable for outpatient treatment. |
| 2 points | Moderate severity; consider short-stay hospital admission. |
| 3-5 points | High severity; requires inpatient management, potentially ICU admission, and parenteral (IV) antibiotics. |
Interventions: Prevention and Treatment
A. Prevention (Crucial for all pregnant women, especially those at risk)
- Influenza Vaccination: All pregnant women should receive an annual inactivated influenza vaccine, regardless of gestational age. This is safe and highly recommended.
- Pneumococcal Vaccination: Recommended for pregnant women at increased risk of pneumococcal disease (e.g., those with chronic heart/lung disease, diabetes, HIV, smoking).
- PCV13 (Prevnar 13): Recommended first, then PPSV23 (Pneumovax 23) later.
- PPSV23 (Pneumovax 23): Can be given, especially if PCV13 is not available.
- Smoking Cessation Counseling: Aggressive counseling and support for pregnant women who smoke.
- Hand Hygiene: Emphasize frequent hand washing to prevent respiratory infections.
- Avoidance of Sick Contacts: Advise pregnant women to avoid close contact with individuals who are sick with respiratory illnesses.
B. Antibiotic Management (Specifics for Pregnancy)
- General Principles:
- Prompt Initiation: Start antibiotics as soon as pneumonia is suspected, ideally after obtaining cultures.
- Avoid Contraindicated Drugs:
- Tetracyclines: (e.g., doxycycline) ABSOLUTELY AVOIDED due to fetal tooth discoloration and bone abnormalities.
- Fluoroquinolones: (e.g., ciprofloxacin, levofloxacin) GENERALLY AVOIDED due to potential for fetal cartilage damage, though data in humans is limited. Use only if no other safe and effective alternative exists.
| Setting | Regimen Details |
|---|---|
| Outpatient Treatment (Mild cases, CURB-65 score 0-1) |
First-line:
|
| Inpatient Treatment (Moderate to severe cases, CURB-65 score 2-5) |
Initial Approach: Start with intravenous (IV) antibiotics. Transition to oral therapy once clinically stable, afebrile, and showing improvement (typically after 48-72 hours). Regimen: An IV Beta-lactam antibiotic combined with a Macrolide. First Choice:
|
| Special Pathogens |
|
C. Supportive Care (Essential for all patients)
- Oxygen Therapy: Maintain SpO2 > 94%. Administer via nasal cannula, face mask, or non-rebreather mask as needed. For severe hypoxia, consider high-flow nasal cannula or non-invasive/invasive ventilation.
- Fluid Management: Maintain adequate hydration intravenously or orally. Be cautious to avoid fluid overload, especially if there's a risk of pulmonary edema.
- Antipyretics: Administer acetaminophen (paracetamol) to control fever, which helps reduce maternal metabolic demand and fetal distress.
- Pain Management: Provide analgesia for chest pain to allow for adequate deep breathing and coughing.
- Bronchodilators: For patients with underlying asthma or significant bronchospasm, inhaled bronchodilators (e.g., albuterol) can be beneficial.
- Positioning: Encourage semi-recumbent or upright positioning to improve lung expansion.
- Respiratory Support: For severe cases, this might include:
- Non-invasive Ventilation (NIV): CPAP or BiPAP to support breathing without intubation.
- Invasive Mechanical Ventilation: If NIV fails or respiratory failure is severe.
- Nutritional Support: Ensure adequate caloric intake, especially if hospitalized for an extended period.
- Deep Vein Thrombosis (DVT) Prophylaxis: Immobilized or critically ill pregnant women should receive prophylactic anticoagulation (e.g., low molecular weight heparin).
- Fetal Monitoring:
- Continuous Fetal Heart Rate (FHR) Monitoring: For moderate to severe cases, to detect fetal distress related to maternal hypoxia or infection.
- Ultrasound: To assess fetal growth, amniotic fluid volume, and well-being, especially if maternal oxygenation is compromised or prolonged illness.
- Management of Complications: Be vigilant for potential complications such as:
- Pleural effusion (fluid around the lungs).
- Empyema (pus in the pleural space).
- Lung abscess.
- Sepsis.
- Preterm labor.
- Fetal distress/hypoxia.
- Maternal acute respiratory distress syndrome (ARDS).
D. Post-Recovery Management
- Follow-up Chest X-Ray: Typically recommended 4-6 weeks after treatment completion to ensure resolution of pneumonia.
- Postpartum Care: Continue monitoring the mother postpartum for any lingering respiratory issues or complications.
- Prevention Counseling: Reiterate the importance of vaccinations and avoiding risk factors for future pregnancies.
INFLUENZA (THE FLU) IN PREGNANCY
Influenza, commonly known as the flu, is a highly contagious respiratory illness caused by influenza viruses. During pregnancy, the physiological changes in a woman's body can make her more susceptible to severe complications from the flu.
Overview & Impact
- The Cause: Influenza is caused by RNA viruses, primarily types A and B.
- How it Spreads: It spreads easily through tiny droplets released into the air when an infected person coughs, sneezes, or talks (aerosolized droplets).
- What it Attacks: The virus primarily infects the ciliated columnar epithelial cells lining the respiratory tract, and in more severe cases, can infect alveolar cells deep within the lungs.
- Incubation Period: Symptoms typically appear 1 to 4 days after exposure.
- Key Message: Pregnant women are a high-risk group for severe influenza complications, including pneumonia, hospitalization, and death.
The 2009 H1N1 Pandemic - A Stark Warning: This pandemic highlighted the severe risks of influenza in pregnancy.
- Pregnant women faced a disproportionately higher risk of severe illness.
- 10% of pregnant women admitted to the hospital with H1N1 required intensive care unit (ICU) admission.
- 11% of those in the ICU unfortunately died.
Diagnosis
Prompt diagnosis is important, especially given the potential for severe outcomes in pregnancy.
- Symptoms: The flu typically presents with a sudden onset of:
- Fever
- Cough
- Sore throat
- Runny or stuffy nose
- Body aches
- Headache
- Fatigue
- Distinguishing from a Common Cold: Flu symptoms are usually more severe and have a more abrupt onset compared to a common cold.
Diagnostic Testing
- Recommended: Reverse Transcription Polymerase Chain Reaction (RT-PCR) or other molecular assays are the preferred tests due to their high sensitivity and specificity. These tests can identify the specific influenza virus type.
- Less Reliable: Rapid influenza diagnostic tests (RIDTs) have lower sensitivity (ranging from 10% to 70%) and can yield false negatives. They should not be used to rule out influenza if clinical suspicion is high.
- When to Test: Consider testing in specific situations:
- If two or more people in a closed setting (e.g., household, childcare) develop influenza-like illness (ILI) with symptom onset within 2-3 days.
- For high-risk individuals, including pregnant women, when treatment decisions depend on confirmed diagnosis.
- To differentiate from other respiratory illnesses, especially during non-flu season.
Management of Influenza in Pregnancy
The goal is to prevent severe illness and complications.
Supportive Care
- Antipyretics: Acetaminophen (paracetamol) is safe and recommended to reduce fever, which helps alleviate maternal discomfort and reduce metabolic demand. Avoid NSAIDs (like ibuprofen) in the third trimester.
- Bed Rest: Encourage rest to aid recovery.
- Hydration: Ensure adequate fluid intake to prevent dehydration.
- Cough Suppressants/Expectorants: Use with caution and consult a healthcare provider. Generally, simple measures like honey and lemon, or saline gargles, are preferred.
Antiviral Treatment: Oseltamivir (Tamiflu)
- Key Principle: Early treatment with Oseltamivir is most effective, ideally started within 48 hours of symptom onset. However, it can still provide benefits even if started later in severe or progressive cases.
- Safety: Oseltamivir is considered safe for use in pregnancy.
- Dosage: The standard dose is 75 mg orally twice daily for 5 days.
Treatment Algorithm for Influenza-like Illness (ILI) in Pregnancy
- If Severe ILI or High-Risk: Immediately start Oseltamivir empirically (without waiting for test results).
- High-risk pregnant women include those with underlying chronic medical conditions (e.g., asthma, diabetes, heart disease).
- If Not Severe ILI: Proceed to step 2.
- 1st Trimester: Perform RT-PCR testing. If positive, initiate individualized treatment with Oseltamivir, considering the risks and benefits. Even in the first trimester, the benefits of treating confirmed flu with Oseltamivir usually outweigh the risks.
- 2nd/3rd Trimester:
- If expected delivery within 7 days: Start Oseltamivir empirically.
- If expected delivery > 7 days: Perform RT-PCR testing first. If positive, start Oseltamivir.
Hospitalization: Consider for pregnant women with severe ILI, signs of pneumonia, respiratory distress, or underlying medical conditions that put them at higher risk.
Prevention: Vaccination is Key!
- Influenza Vaccine (Flu Shot):
- Safety & Recommendation: The inactivated influenza vaccine (flu shot) is safe and strongly recommended for all pregnant women in every pregnancy, regardless of gestational age (any trimester).
- Benefits:
- Significantly reduces the risk of respiratory illness in the mother (by about half).
- Reduces the risk of hospitalization for flu-related complications by approximately 40%.
- Provides crucial passive immunity to the newborn for several months after birth, as maternal antibodies are transferred across the placenta.
- Tdap Vaccine:
- Recommendation: Also recommended for all pregnant women between 27 and 36 weeks of gestation (ideally early in this window) to protect the newborn from pertussis (whooping cough).
- Importance: This is a separate vaccine but often given during the same pregnancy for maternal and neonatal protection.
COVID-19 IN PREGNANCY:
COVID-19, caused by the SARS-CoV-2 virus, has presented unique challenges during pregnancy. Understanding its impact and appropriate management is vital.
Pathophysiology & Increased Vulnerability in Pregnancy
- The Virus: SARS-CoV-2 is the causative agent.
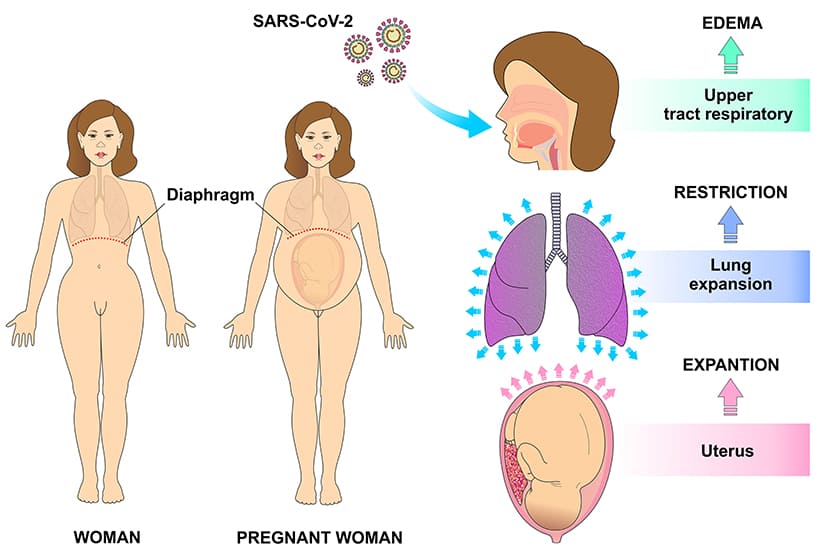
- Respiratory Changes: Pregnancy itself leads to physiological changes that can exacerbate respiratory infections:
- Mechanical Changes: The growing uterus elevates the diaphragm, reducing lung capacity.
- Hormonal Influence: Estrogen-dependent progesterone receptors in the hypothalamus stimulate the respiratory center, leading to increased respiratory drive but also a sensation of dyspnea.
- Immunological Shift: Pregnancy is associated with an immunological shift from a pro-inflammatory Th1-type response to a more anti-inflammatory Th2-type response to prevent rejection of the fetus. While beneficial for pregnancy, this shift can impair the immune system's ability to effectively fight off viral infections like SARS-CoV-2.
- Compromised Mucociliary Clearance: The natural ability of the respiratory tract to clear mucus and pathogens can be reduced.
- Third Trimester Risk: Pregnant women in their third trimester are at particularly high risk for more severe COVID-19 due to these combined factors, including rapid viral multiplication and compromised lung mechanics.
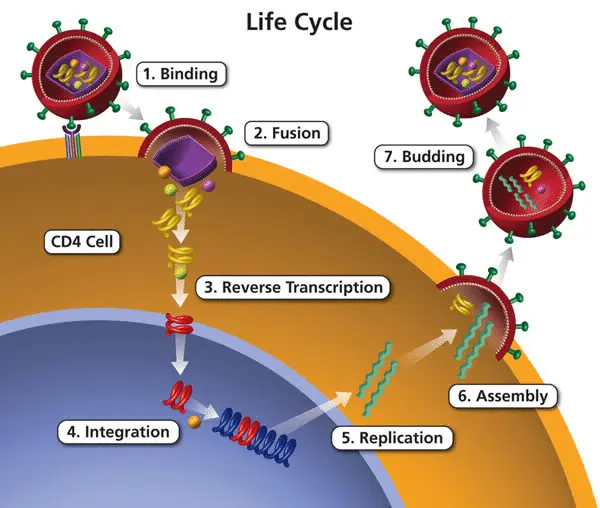
- ACE2 Receptors:
- Role: SARS-CoV-2 enters human cells by binding to the Angiotensin-Converting Enzyme 2 (ACE2) receptor.
- Pregnancy Implication: ACE2 receptors are found in various maternal and fetal tissues and are upregulated (increased in number) during pregnancy. This might contribute to the unique susceptibility or disease course in pregnant individuals.
- Angiotensin II: Activation of the Renin-Angiotensin-Aldosterone System (RAAS) and subsequent increase in Angiotensin II can lead to vasoconstriction (narrowing of blood vessels) and thrombosis (blood clot formation), which are prominent features of severe COVID-19.
Symptoms: COVID-19 vs. Common Cold vs. Flu
| Symptom | COVID-19 | Common Cold | Flu |
|---|---|---|---|
| Fever | Common | Rare | Common, abrupt |
| Dry Cough | Common | Common | Common |
| Sore Throat | Common | Common | Common |
| Runny/Stuffy Nose | Common | Common | Common |
| Body Aches/Headache | Common | Mild | Common, severe |
| Fatigue | Common, can be severe | Mild | Common, severe |
| Loss of Taste/Smell | Specific, common | Rare | Rare |
| Shortness of Breath | Sometimes (can be severe) | Never | Sometimes |
| Diarrhea | Sometimes | Rare | Sometimes |
Complications in Pregnancy
Pregnant women with COVID-19 are at increased risk for several adverse outcomes:
- Maternal:
- Pneumonia: More frequent and often more severe, requiring oxygen support or mechanical ventilation.
- Thromboembolic Events: Increased risk of blood clots (e.g., DVT, pulmonary embolism).
- Preeclampsia: Some studies suggest a higher risk of developing this pregnancy-specific hypertensive disorder.
- Gestational Diabetes: Potential increased risk.
- Need for ICU Admission/Mechanical Ventilation.
- Maternal Mortality.
- Fetal/Neonatal:
- Preterm Delivery: The most common adverse perinatal outcome, often for maternal indications (e.g., severe maternal illness, need for urgent delivery).
- Fetal Growth Restriction (FGR).
- Stillbirth: Slightly increased risk.
- Neonatal Intensive Care Unit (NICU) Admission.
- Severe diarrhea: Can occur in neonates if infected.
Vertical Transmission (Mother to Baby)
Overall Conclusion: While possible, vertical transmission is considered rare and not the primary mode of neonatal infection. Most neonatal infections occur post-natally from exposure to infected caregivers.
- Conflicting Evidence: Some studies found negative results (no virus in cord blood), while others suggest possible in utero transmission via elevated IgM/IgG antibodies or viral RNA in placental tissue.
- Elevated inflammatory cytokines in the placenta suggest an inflammatory response potentially triggered by the virus.
Management Protocol
- Asymptomatic or Mild Cases:
- Home Isolation: 14 days of isolation.
- Monitoring: Regular self-monitoring of symptoms, temperature, and oxygen saturation. Tele-consultations with healthcare providers are encouraged.
- Supportive Care: Rest, hydration, acetaminophen for fever if needed.
- Symptomatic Cases:
- Negative Test: If symptoms persist or worsen, continue home isolation and close monitoring. Consider re-testing or investigating other causes.
- Positive Test (Moderate to Severe Symptoms):
- Hospitalization: Recommended in a tertiary care center.
- Maternal Surveillance: Monitor vitals (including SpO2) 3-4 times per day. Chest imaging (X-ray/CT with shielding). Regular labs (CBC, LFTs, inflammatory markers).
- Thromboprophylaxis: Prophylactic anticoagulation (e.g., LMWH) is usually initiated due to thrombosis risk.
- Fetal Surveillance: Continuous/frequent FHR monitoring. Corticosteroids for fetal lung maturation if preterm delivery is anticipated (24-34+6 weeks). IV Antibiotics if bacterial co-infection suspected.
Pregnant women meeting these criteria require immediate ICU transfer.
- Systolic Blood Pressure (SBP) < 100 mmHg
- Respiratory Rate (RR) > 22 breaths/minute
- Glasgow Coma Scale (GCS) < 15 (indicating altered mental status)
Indications for Considering C-Section in Severe Failure:
- Septic Shock: Unresponsive to fluids and vasopressors.
- Acute Organ Failure: Progressive respiratory failure (ARDS), renal failure, cardiac dysfunction.
- Fetal Distress: Persistent non-reassuring fetal status despite optimal maternal resuscitation.
- Note: The decision to deliver should be individualized, balancing maternal and fetal conditions.
Vaccination (COVID-19)
- Global Consensus: Organizations like FIGO and FOGSI recommend COVID-19 vaccination for pregnant and breastfeeding women.
- Benefits Outweigh Risks: Vaccination significantly reduces severe illness, hospitalization, and death.
- Safety & Efficacy: Studies show vaccines are safe in pregnancy.
- Breastfeeding: No known adverse effects on the neonate. Potential passage of protective antibodies (IgA and IgG) through breast milk offers passive immunity.
ACUTE LUNG INJURY (ALI) & ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) IN PREGNANCY
Acute Lung Injury (ALI) and its more severe form, Acute Respiratory Distress Syndrome (ARDS), are life-threatening conditions characterized by severe inflammation and fluid accumulation in the lungs, leading to profound hypoxemia.
Definitions & Criteria
The Berlin Definition (2012) is now the universally accepted standard for ARDS. The term ALI has largely been subsumed within a graded severity of ARDS.
ARDS [Berlin Definition 2012 - Current Standard]:
- Timing: Within 1 week of a known clinical insult or new or worsening respiratory symptoms.
- Chest Imaging: Bilateral opacities (infiltrates), not fully explained by effusions, lobar/lung collapse, or nodules.
- Origin of Edema: Respiratory failure not fully explained by cardiac failure or fluid overload.
- Oxygenation Impairment (PaO2/FiO2 ratio with PEEP/CPAP ≥ 5 cmH2O):
- Mild ARDS: PaO2/FiO2 between 200 mmHg and 300 mmHg.
- Moderate ARDS: PaO2/FiO2 between 100 mmHg and 200 mmHg.
- Severe ARDS: PaO2/FiO2 < 100 mmHg.
Pathophysiology: The Cascade of Damage
- Diffuse Alveolar Damage (DAD): The hallmark pathological finding. Initial insult triggers systemic inflammation.
- Endothelial and Epithelial Damage: Damage to the alveolar-capillary membrane leads to increased permeability (leakiness).
- Increased Permeability: Protein-rich fluid, neutrophils, and red blood cells flood alveolar spaces.
- Neutrophilic Inflammation: Release of proteases and cytokines causes further damage.
- "Hyaline Membrane" Formation: Glassy membranes line alveolar walls, impeding gas exchange.
- Collapsed Airspace (Atelectasis): Loss of surfactant leads to alveolar collapse.
- V/Q Mismatch & Shunt: Alveoli are perfused but not ventilated, causing profound hypoxemia.
Causes in Pregnancy: A Diverse Etiology
- Incidental (Non-Obstetric) Causes:
- Sepsis (Most common cause), Severe Pneumonia (Viral/Bacterial), Aspiration Pneumonitis, Trauma, Pancreatitis, Drug Overdose, Massive Transfusion (TRALI).
- Exacerbated by Pregnancy:
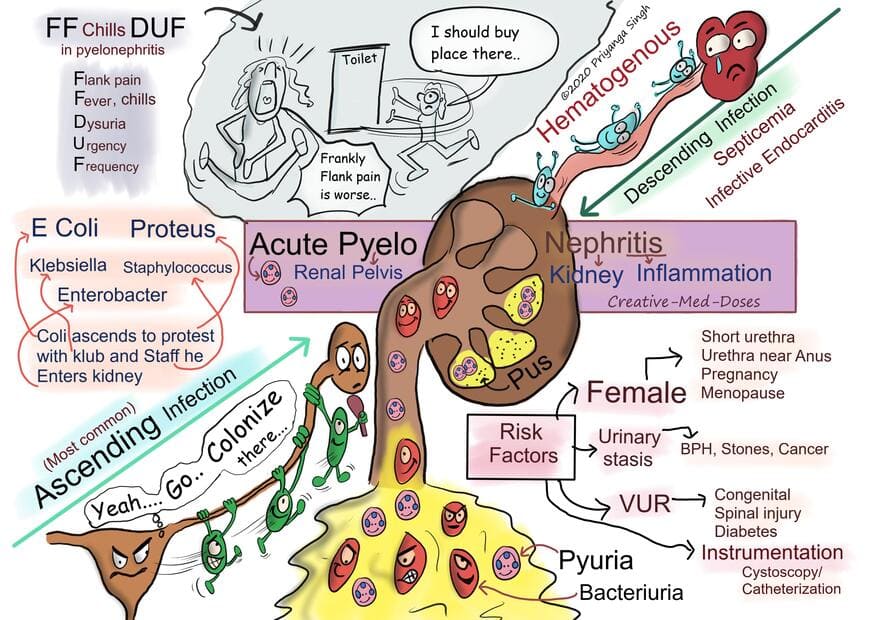
- Aspiration (Mendelson's Syndrome), Pyelonephritis (Sepsis source), Viral Pneumonia.
- Unique to Pregnancy (Obstetric) Causes:
- Preeclampsia/HELLP Syndrome.
- Tocolytic-induced Pulmonary Edema.
- Amniotic Fluid Embolism (AFE).
- Placental Abruption (Massive hemorrhage/DIC).
Management of ARDS in Pregnancy
Requires a highly coordinated, multidisciplinary team (Obstetrician, Neonatologist, Intensivist, Pulmonologist, Anesthesiologist).
Emergency Steps (ABCs of Resuscitation):
- Airway: Secure the airway. Endotracheal intubation is indicated for unconsciousness, unprotected airway, or severe hypoxemia (e.g., PaO2 < 60 mmHg, SpO2 < 90%).
- Breathing: Provide ventilatory support.
- Non-Invasive (NIPPV): Can be tried in early/mild ARDS if stable.
- Invasive (IPPV): Required for established ARDS. Goal is to maintain SpO2 > 95% (maternal target) to optimize fetal oxygenation.
- Circulation: Maintain adequate cardiovascular function. Target Mean Arterial Pressure (MAP) > 65 mmHg to ensure placental perfusion.
Mechanical Ventilation Strategy (Lung Protective Ventilation)
This is the cornerstone of ARDS management.
- Low Tidal Volume (Vt): Set at 6 ml/kg of predicted body weight to prevent volutrauma.
- Plateau Pressure (Pplat): Keep Pplat < 30 cm H2O.
- Permissive Hypercapnia: Allow PaCO2 to rise (target < 45-50 mmHg) to achieve low tidal volumes. Caution in pregnancy: Severe acidosis (pH < 7.2) is poorly tolerated by the fetus.
- Positive End-Expiratory Pressure (PEEP): Apply PEEP (5-15 cmH2O) to keep alveoli open.
- Maternal Oxygenation Goal: Maintain PaO2 > 65 mmHg and SpO2 > 95%.
Other Management Strategies
- Fluid Management (FACTT Protocol): Conservative/Restricted fluid strategy ("dry lung" approach). Aim for CVP < 4 mmHg. Use diuretics as needed.
- Positioning:
- Prone Positioning: Standard for adult ARDS but difficult in advanced pregnancy.
- Left Lateral Decubitus (LLD): Often preferred to reduce uterine compression on the inferior vena cava.
- Head of Bed Elevation: 30-45 degrees to improve lung mechanics.
- Medications:
- Corticosteroids: Routine use not recommended for ARDS, but antenatal steroids for fetal lung maturation are indicated if preterm delivery anticipated.
- Neuromuscular Blockers: Used for deep sedation in severe ARDS.
- ECMO: For severe, refractory ARDS.
- DVT Prophylaxis: Mechanical and pharmacological prophylaxis (LMWH).
- Nutrition: Early enteral nutrition via feeding tube.
- Glycemic Control: Strict blood glucose control.
Scoring Systems for Prognosis
- APACHE II/III: Predicts mortality based on physiological measurements and age.
- SAPS II: Simplified Acute Physiologic Score.
- SOFA (Sequential Organ Failure Assessment): Tracks organ failure across 6 systems. qSOFA used for rapid sepsis assessment.
Fetal Considerations in ARDS
- Fetal Distress due to Maternal Hypoxemia: Primary concern.
- Preterm Labor: Can be triggered by stress/infection.
- Delivery Decisions: Complex and individualized.
- General Rule: Delivery is generally not indicated solely for maternal ARDS unless the fetus is compromised, or delivery is part of the treatment for the underlying cause (e.g., severe preeclampsia). Aggressive maternal resuscitation is usually the priority.
- Mode: C-section often chosen if urgent/unstable; vaginal if stable.
- Get Vaccinated: Flu, COVID-19, Pneumococcal.
- Hygiene: Wash hands, avoid crowds, wear masks in crowded settings.
- Ventilation: Ensure good indoor air flow.
- Health: Manage chronic conditions (asthma/diabetes) and avoid smoking.
Respiratory Tract Infections in Pregnancy Read More »