Guide to the Question Approach for Midwifery Exams
It is important for midwives preparing for the exam to be able to answer questions effectively.
This approach allows you to tackle questions in a systematic manner, ensuring that you cover all important points and provide concise and accurate answers. By following this structured approach, you will be able to effectively demonstrate your knowledge, critical thinking and analytical skills, leading to higher scores and overall success on your midwifery exams.
Whether you are facing questions that require you to EXPLAIN, OUTLINE, DESCRIBE, MENTION, IDENTIFY, STATE, LIST, WHAT and GIVE, this article is all you need!
Explaining Questions: Breaking Down Complex Concepts
When questions require explanations, it is essential to break down complex concepts into understandable parts. Start by introducing the topic you’re discussing and providing a concise definition if necessary. Then, proceed to explain on the key components or factors related to the topic. Use clear and simple language to ensure your explanation is easily understandable.
Example Question: Explain how you would admit a mother who has reported in active phase of first stage?
In response to this question, you can follow the question approach by giving the key points step by step:
- Reception: the mother and the relatives are welcomed; mother is taken to the admission room while the relatives are offered seats. Rapport between the mother, attendants and the midwives is created.
- History taking: if the mother has been attending ANC, her ANC record is obtained; to get the history and any risk factors like multiple pregnancies. If she has not been attending ANC, a full antenatal history is taken, which involves the mother‘s name, address, tribe, religion, husband‘s name and address, her gravida and parity, obstetrical, surgical, social, and medical history, the time and date of admission are entered in the admission forms of the mother.
Then, history of labour under the following headings is recorded:
- Show: the mother is asked if she has seen any blood and mucus, her undergarments examined for any stain, vulva examined for the drainage of show which may appear a few hours before or after beginning of labour.
- Uterine contractions: mother is asked when the regular pains began, how often and if she has backache. Her statement about the length, severity, or expulsive character of the contraction should be confirmed by observation and evaluation then
- Membranes: She is asked whether her water (amniotic fluid) have ruptured or not; if she has noticed a gush or tickling of water → the amount and time are recorded. If in doubt of whether its liquor or urine, litmus paper is dipped into the draining fluid obtained from the vulva to confirm alkalinity or
- Vaginal discharge or bleeding: the mother is also asked if she had any vaginal bleeding/ discharge which should be excluded
- General examination of the mother: her general appearance is noted, that is healthy or ill, colour, any deformities like lame, presence of oedema, infections, varicose veins or enlarged neck veins. Breast examination is carried out to identify their sustainability for breast feeding
- Observations; Vital signs are monitored like temperature, pulse, respiration and blood pressure to rule out eclampsia in She is also asked for bowel action, sleep and rest
- Abdominal Examination: first, the bladder should be empty and this is carried out with the mother lying on the couch on supine position with a pillow under her head and This examination is carried out as follows:
- On inspection: the shape of the abdomen is noted whether round or oval, the size should be correspond with the weeks of gestation, the foetal movements, skin changes like stria gravidarum and linea nigra and any scar are
- On palpation: this can be superficial, fundal, lateral, pelvic, height of the fundus and hypochondriac. They are carried out to note the lie whether its longitudinal, transverse, or oblique; the position of the fetus which can be ROA, LOA, ROP, LOP; and engagement plus enlargement of the spleen and the liver.
- On auscultation: the fetal heart is listened, if its heard and regular
- Vulva shave, toilet and examination: the shave is done on women whose cultures allow keeping the vulval area with pubic hair. Any abnormal discharges, oedema, or paleness are noted if present
- Vaginal examination: this is done to mothers who have no history of APH with the current pregnancy under strict asepsis. It‘s done to confirm the onset of labour, the presentation, position, engagement, station of the presenting part, to confirm whether membranes ruptured or intact, exclude cord prolapsed, assess the pelvis if adequate or inadequate and also progress of labour and it‘s the one that determines the admission of a mother on the partograph
- Investigations: routine samples are obtained for example:
- Blood: for routine counseling and testing (RCT), rapid polymerase reaction (RPR), HBsAg, haemoglobin estimation, Grouping and cross matching → rational to confirm presence of any disease so as to prevent mother to child transmission (MTCT) and for blood transfusion (BT) in case of anaemia
- Urine: for analysis to test for albumin, sugar, acetone that might complicate labour
- Personal hygiene: a shower is both hygienic and pleasant. If the mother‘s membrane have ruptured or in advanced first stage of labour, she is sponged down on a couch and given a clean
Admission: the mother is then admitted on a partograph, all the necessary information recorded and the continuous observation of the mother takes place accordingly
Outlining Questions: Structuring Information
When faced with outlining questions, it is important to structure your response in a logical and organized manner. Begin by providing an the main points or components related to the topic. Use subheadings to break down the information further, making it easier for the examiner to follow your answer.
Example Question: Outline the changes that take place in the uterus during the first stage of labour?
Before answering the proposed question above, it‘s vital to first define the following terms:
- Labour: is the process by which the foetus, placenta and the membranes are expelled out of the birth canal after 28th weeks of gestation
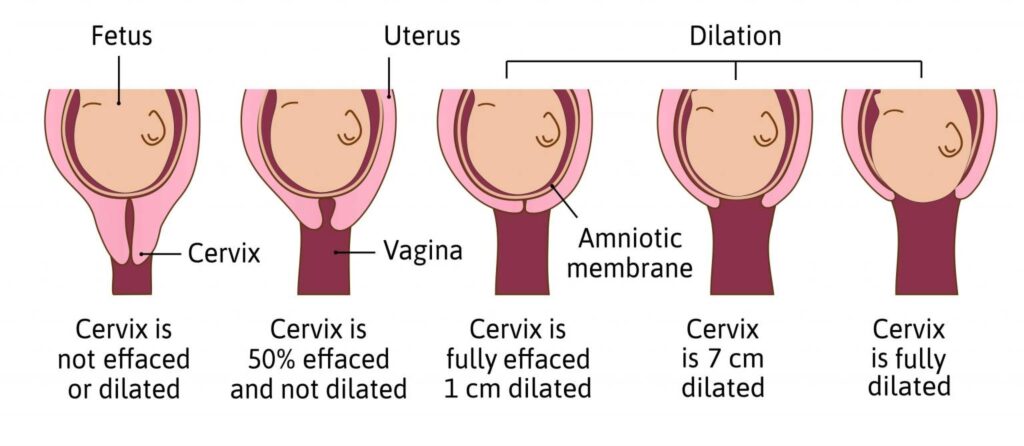
- First stage of labour: is the period of dilatation of the cervix lasting from the onset of true labor till full dilatation.
During the first stage of labour the following occurs:
- Effacement or take up of the cervix: this is made possible by the work of muscle fibres surrounding the internal OS which are drawn upward by the retracted upper segment.
- Pacemaker / Fundal dominance: each contraction begins from the pace maker situated at the cornua of the uterus. From the fundal region it spreads downwards being stronger and persisting longer in the upper region on reaching the lower region, the wave of contraction weakens and allows the cervix to dilate.
- Dilatation of the cervix: this is the opening of the external OS to allow the passage of the fetal head; it occurs as a result of uterine action and the pressure from fore bag of waters and the well fitting presenting part
- Contraction and Retraction: is the special ability of the uterine muscle where the contraction does not pass off completely and the muscle fibres, retaining some of the contractions, do not become completely relaxed, instead they become gradually shorter and thicker.
- Polarity: is the term used to define the coordination between two poles of uterus throughout labour.
- Development of upper and lower segment: the upper uterine segment is the thicker muscular contractile part. The lower part segment is the firm distensible are of 7.5cm – 10cm in length developed from isthmus to the uterus.
- Development of retraction ring: is the ridge formed between the upper and the lower uterine segment. It‘s present in labour and normal as long as it‘s not marked enough to be visible above the symphysis pubis. NB: It is called bandl‘s ring in obstructed labour
- Show: is the blood stained mucoid discharge seen a few hours within or a few hours after when labour has started.
- General fluid pressure: while the membranes remain intact, the pressure of the uterine contraction is exerted on the fluid as the fluid is not compressible the pressure is equalized throughout the uterus.
- Rupture of membranes: rupture of membranes may be early or later during the second stage of labour due to the malpresentation and pressure from the presenting part.
- Fetal axis pressure: this is when the force of contractions from the uterus is transmitted via the long axis of the canal; this becomes more significant after the rupture of membranes and during second stage.
Describing Questions: Providing Detailed Information
Describing questions require you to provide detailed information about a specific topic or concept. When answering these questions, you have to offer a comprehensive and thorough response, including relevant facts, characteristics, and examples. Use clear language and provide specific details to enhance the depth of your description.
Example Question: Describe the vagina.
Definition: Vagina is a muscular fibrous canal which forms the part of the internal female reproductive organs.
Situation: It is a canal which extends from the vestibule below to the cervix above running in an upward and backward direction between the planes of the pelvic brim.
Shape: It is a potential tube which runs upwards and backwards with its walls in close contact but can be separated during coitus, menstruation, vaginal examination and child birth.
Size: The anterior wall measures 7.5cm. The posterior wall is longer and it measures 10cm.This is because the uterus enters the vagina at an angle of 90 degrees and bends forwards towards the anterior wall hence it encroaches on it
Structure
Gross structure
Superiorly; the upper end of the vagina is known as the vault, where the cervix protrudes into the vault it forms circular recess known as fournices.
The vagina is made up of four fournices that is to say;
- The anterior fornix which is smaller and fairly deep The 2 lateral fournices which are shallow
- The posterior fornix which is the longest and deepest
- The lower end of the vagina is narrow and inferiorly we find the vulva, hymen enclosing the vaginal opening only present in virgins. If hymen is ruptured it leaves tags of membranes referred to as carunculae mytiformes. Vaginal orifice is also called introitus.
Microscopic structure
It is made up of four layers;
- Squamous epithelium arranged in folds known as rugae and makes the inner most layer of the vagina, the rugae increase the surface area and offer the vagina ability to stretch when need be for example during coitus and child bearing.
- Vascular connective tissue layer which is rich in blood vessels, nerves and lymphatics and is found just beneath the epithelium.
- Muscular layer. This is thin but a strong layer which is divided into two; the weak inner circular and strong outer longitudinal fibres.
- The pelvic fascial which is made up of loose connective It forms the outer protective coat and is continuous with the pelvic fascia.
Blood supply (arterial): The vagina is supplied by the branches of internal iliac artery which include vaginal artery and uterine artery.
Venous drainage: By the corresponding veins i.e branches of internal iliac veins which include vaginal veins and uterine veins.
Lymphatic drainage: Into the inguinal, the iliac and the sacro glands
Nerve supply: By the sympathetic and parasympathetic nerves which are branches from the lee Franken lanser plexus
Contents of the vagina
- It doesn‘t contain any glands but its kept moist by cervical mucus and a transudation from the underlying blood vessels through the epithelium.
- Its media is acidic (PH 3.8 to 4.5) and this is made possible by presence of lactic acid after action of doderleins bacilli on glycogen.
Relationships of the vagina
Anteriorly: Below, the base of the bladder rests on the upper ½ of the vagina and the urethra is embedded in the lower ½.
Posteriorly: Pouch of Douglas above, the rectum medial and perineal body below.
Laterally: Pubococcygeous muscles below and pubic fascial containing the uterus above.
Inferiorly: The structure of the vulva.
Superiorly: The cervix and the fournices.
Functions of the vagina
- Exit from menstrual flow.
- Entrance for spermatozoa.
- Exit for products of conception.
- Supports the uterus.
- Prevents ascending infection due to acidic PH.
- For assessing the pelvis.
- Drug administration.
Mentioning, Identifying, and Stating Questions: Being Clear and Concise
When faced with questions that require you to mention, identify, or state specific information, it is essential to be clear, concise, and accurate in your response. Avoid unnecessary elaboration and focus on providing the requested information directly.
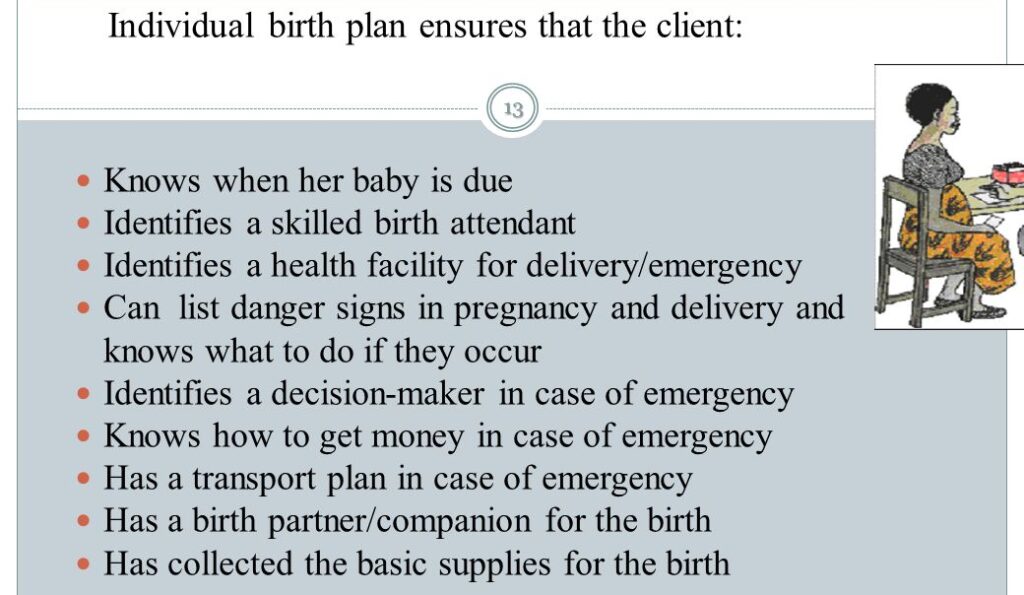
Example Question: State the major components of a comprehensive birth plan?
To answer this question effectively, you can provide a concise statement listing the major components of a birth plan:
A comprehensive birth plan typically includes the following components:
- Preferred birth environment (hospital, birthing center, home birth)
- Pain management preferences (medication, natural methods, water birth)
- Support people and their roles during labor and delivery(husband, mother)
- Positioning preferences for labor and birth(lithotomy)
- Preferences for fetal monitoring during labor
- Neonatal interventions and care preferences immediately after birth
- Feeding preferences (breastfeeding, formula feeding)
- Cultural or religious considerations
- Preferences for postpartum care and rooming-in with the baby
- Contingency plans for unexpected situations or interventions
By providing a clear and concise statement of the major components, you address the question directly and effectively.
Listing and Giving Questions: Providing Comprehensive Information
When asked to list or give information, it is important to provide a response that covers all the relevant points. Ensure that you include all necessary information without leaving out any key details.
Example Question: List and give examples of common obstetric emergencies that midwives may encounter?
In response to this question, here is a comprehensive list of common obstetric emergencies along with examples:
Postpartum Hemorrhage (PPH): This is excessive bleeding following childbirth. Examples include uterine atony (lack of uterine contractions), retained placenta, or trauma to the birth canal.
Shoulder Dystocia: It occurs when the baby’s shoulders become stuck behind the mother’s pubic bone during delivery. This can lead to complications such as brachial plexus injury or fetal hypoxia.
Umbilical Cord Prolapse: The umbilical cord slips through the cervix ahead of the baby, potentially cutting off the baby’s oxygen supply. This requires immediate action to relieve pressure on the cord.
Amniotic Fluid Embolism: This is a rare but life-threatening condition where amniotic fluid enters the mother’s bloodstream, triggering an allergic reaction. It can result in cardiac arrest, respiratory failure, or disseminated intravascular coagulation (DIC).
Pre-eclampsia/Eclampsia: Pre-eclampsia is characterized by high blood pressure and organ damage during pregnancy, while eclampsia is the development of seizures in a woman with pre-eclampsia.
Placental Abruption: This occurs when the placenta separates from the uterine wall before delivery. It can cause severe bleeding and compromise fetal oxygen supply, necessitating emergency delivery.
Fetal Distress: This refers to a compromised fetal condition during labor, usually due to inadequate oxygen supply. It may require interventions such as changing maternal positions, administering oxygen, or performing an emergency cesarean section.
Cord Compression: The umbilical cord becomes compressed during labor, restricting blood flow to the baby. This can occur due to cord entanglement, excessive cord length, or abnormal positioning.
Maternal Infections: Infections such as chorioamnionitis (infection of the placental membranes), sepsis, or genital tract infections can pose risks to both the mother and the baby.
Maternal Hypertensive Disorders: These include gestational hypertension, chronic hypertension, and HELLP syndrome.
Write Short Notes: Concise and Informative Summaries
When encountering “Write Short Notes” questions, the aim is to provide concise yet informative summaries of the given topic. These questions require you to summarize the key points and present them in a clear and organized manner. Avoid excessive details and focus on providing a brief but comprehensive overview.
Example Question: Write short notes on the following
(a) Causes of pain in labour.
(b) Factors that affect pain perception during labour.
(a)CAUSES OF PAIN
There are two major causes of pain
- Hormonal factors
- Mechanical factors
Hormonal factors These include;
Oxytocin stimulation. This increases the strength, intensity, duration and frequency of the contractions leading to pain.
Progesterone withdrawal. The reduced levels of progesterone lead to an increase in estrogen levels which stimulates the muscles of the deciduae muscles of the uterus to produce prostaglandin which stimulates the smooth muscles of the uterus to contract.
Mechanical factors These include;
Strength and frequency of Braxton hick‘s contractions occurring in late pregnancy which leads to over stretching of the uterus which irritates the uterine muscles to contract leading to pain.
Pressure of the presenting part on the sacro-nerves and lumbar nerves which has pain receptor.
Pressure of the presenting part on the cervix. The presenting part exerts pressure on the cervix muscles hence leading to pain.
Displacement of the pelvic floor muscles. The advancing presenting part distends the vagina and displaces the pelvic floor muscles which are over stretched and the nerves are compressed leading to pain.
(b) PERCEPTION.
Is the process of becoming aware of the environment through the five senses.
Factors that affect pain perception during labour
These factors are emotional experience involving physical and psychological mechanism and can be contributed by the mother, fetus, health workers and structural environment.
Mother
- Maternal medical; conditions like pre-clampsia and eclampsia, cardiac conditions which can affect pain perception.
- Compromised immunity due to chronic conditions like HIV and cancer which can affect pain perception.
- Size of the pelvis. Any pelvic deviation from normal leading to cephalous pelvic disproportion which can affect pain perception.
- Age. Young prime gravidae below 18years their pelvic bones are not fully developed and the mother above 35years their pelvic bones are contracted and this hinders normal progress of labour and affects pain.
- Parity. Prime gravidae‘s their muscles are still intact and sensitive to pain which leads to strong contractions. The multipara mothers their muscles are laced which leads to uterine itial.
- Past obstetrical history like caesarian section which increases the risks of uterine rapture and affects normal labour
- Social economic factors for example lack of support which can affect pain perception.
- Cultural factors like use of native drugs can affect pain perception.
- Past experience can also affect pain perception
- Level of education, occupation, religion can also affect pain perception.
Fetus
- Fetal abnormalities like hydrocephalous, macrosomic babies can lead to cephalopelvic disproportion hence affecting pain.
- Lie, position and presenting pain can affect pain perception during labour
- Size of the fetus that is to say big babies which cannot pass through the pelvis hence affecting pain perception
- Gestation age. In past maturity the sutures and the fontanels are closing and molding can hot take place hence affecting pain perception.
Health workers
- Poor screening of mothers during antenatal Poor management during labour
- Poor attitude towards the mother
Structural environment
- Hospital setting where there is no privacy for mothers, all stages of labour in one room which can affect pain perception.
- Lack of recreation in labour rooms like newspapers, television to occupy the mothers.
What Questions: Providing Clear Definitions and Explanations
“What” questions typically require you to provide clear definitions, explanations, or descriptions of a specific concept, procedure, or pathophysiology These questions aim to test your understanding and knowledge of the subject matter. When answering “What” questions, it is important to be precise and concise in your response, while still providing sufficient information to address the question accurately.
Example Question: What is the role of the midwife in the immediate postpartum period?
To answer this question effectively, you can provide a concise definition and description of the midwife’s role during the immediate postpartum period:
Monitoring maternal and neonatal vital signs: Midwives closely monitor the mother’s blood pressure, heart rate, and bleeding. They also assess the baby’s breathing, heart rate, and overall well-being.
Assisting with breastfeeding initiation: Midwives provide support and guidance to initiate breastfeeding, ensuring proper positioning. They offer education on breastfeeding techniques, addressing any concerns or difficulties that may arise.
Providing emotional support: Midwives offer emotional support to new mothers, addressing any anxieties, fears, or questions they may have. They create a nurturing and supportive environment for the mother and her newborn.
Assessing postpartum recovery: Midwives conduct physical examinations to assess the mother’s postpartum recovery, including uterine involution, healing of perineal tissues, and overall well-being. They provide guidance on self-care practices and postpartum contraception options.
Identifying and managing postpartum complications: Midwives are identify and manage any postpartum complications that may arise, such as postpartum hemorrhage, infection, or breastfeeding difficulties. They collaborate with healthcare providers if further interventions are required.
By explaining the midwife’s role in the immediate postpartum period, you address the “What” question while providing a clear understanding of the topic.
What information must you note on vaginal examination?
On inspection
State of the vulva, note any abnormal discharges like pus, blood, abnormal growths like warts, oedema and scars.
On examination
- Note condition of the vagina. Normally the vaginal walls feel warm and moist and dilatable. If dry may be a sign of infection or obstruction.
- State of the cervix. If thin, thick, whether soft or rigid and whether its well applied to the presenting part. Note dilatation and cervical effacement.
- State of the membranes. Whether intact or ruptured. If ruptured check colour and smell of liquor
- Presentation and presenting part. Note level of presenting part in the pelvis. Confirm position by finding or palpating sutures and fontanelles and relate them to the maternal pelvis. Note moulding.
- Do internal pelvic assessment and note
- -sacro promontary if protruding
- -hollow of the sacrum if well curved
- -sciatic notches if well rounded
- -ischial spines if prominent
- -sub pubic arch-if it accommodates 2 ½ to 3 fingers
- -inter tuberous diameter if it accommodates 4 knuckles
Tips for Success:
a. Understand the instructions: Carefully read and follow the instructions.
b. Plan your response: Take a moment to brainstorm and outline your ideas before starting to write. This will help you organize your thoughts and ensure a great structured response.
c. Provide relevant examples: Whenever possible, support your answers with real-life examples, or evidence-based practices to demonstrate your understanding and application of midwifery knowledge.
d. Use clear and simple language: Write in a clear and simple manner, avoiding unnecessary elaboration. Focus on delivering information effectively while maintaining clarity.
e. Practice time management: Allocate time for each question based on its difficulty. This will help you ensure that you have enough time to answer all questions within the given time.
f. Review your answers: Before submitting your answer sheet, review your answers to check for any errors, omissions, or areas that need further clarification or elaboration. Don’t forget to write your NSIN Number!