
Physiology of Pregnancy
1. Changes in the Endocrine System (Hormones)
The placenta produces several hormones that cause many physical changes. The successful adjustment of the mother's body is made possible by changes in hormone production by the mother's endocrine system and the trophoblast (the outer layer of cells of the early embryo).
- Human Chorionic Gonadotropin (HCG): This hormone is produced by the trophoblast. HCG levels increase very fast in early pregnancy, reaching their highest levels at 8 to 10 weeks of gestation. The main job of HCG is to keep the corpus luteum working so it can keep producing Progesterone and Oestrogen. It does this until the placenta is ready to produce enough hormones on its own (around 10 to 12 weeks). After that, HCG levels slowly drop until it completely disappears 2 weeks after birth.
- Progesterone Hormone: This is mainly produced in the corpus luteum in the beginning. Its job is to make the lining of the uterus (decidua) thick, soft, and ready to receive the fertilized egg. It also helps to increase the glandular tissue and milk ducts in the breasts, and the muscle fibers in the uterus.
- Oestrogen: This hormone causes the uterus to grow and also develops the duct system in the breasts during pregnancy. It is passed out of the body in the urine, and measuring the amount of oestrogen in the urine can show how well the baby is doing (fetal wellbeing).
- Relaxin Hormone: During the last few weeks of pregnancy, this hormone acts on the ligaments and joints, making the pelvis relax and "give" way for the baby to pass. It is also produced by the decidua and the trophoblast to help the uterine muscles (myometrium) relax. It also plays a role in softening the cervix and breaking the water membranes.
- Human Placental Lactogen (HPL): This hormone stimulates breast growth and helps prepare the breasts for making milk (lactogenic properties). It also causes metabolic changes that make sure plenty of glucose (sugar) is available for the growing baby's brain and body, protecting the baby from poor nutrition.
- Pituitary Hormones: The Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH) are stopped from working because of the high levels of Oestrogen and Progesterone. The adrenal gland only grows slightly in size, but it increases its hormone production.
- Thyroid Function: In a normal pregnancy, the thyroid gland gets bigger because its tissue grows and it gets more blood supply. The body takes up more iodine during pregnancy to make up for the iodine lost through the kidneys, which stops the blood iodine levels from dropping too low.
2. Changes in the Reproductive System
Changes in the Uterus
The uterus stretches and expands greatly to make room for and feed the growing baby. This growth happens in the middle muscle layer called the myometrium. The body of the uterus grows to create a safe, feeding environment for the baby to develop.
Uterine Muscle Layers
- 1. Endometrium: Menstruation completely stops. During pregnancy, this inner lining is called the decidua. It becomes very thick, soft, spongy, and gets a very rich blood supply.
- 2. Myometrium (Muscle Layer): The growth of the uterus body is caused by two main factors:
- Hypertrophy: The actual muscle fibers increase in size. They become about 10 times longer and 3 times wider.
- Hyperplasia: New muscle cells are created and grow next to the original muscle cells. This means an increase in the total number of cells.
Size, Weight, and Shape Changes:
- Size and Weight: Before pregnancy, the normal uterus is 7.5cm long, 5cm wide, and 2.5cm thick, weighing just 60g. By the end of pregnancy, it becomes 30cm long, 23cm wide, and 20cm thick, weighing a massive 960g.
- Shape: A healthy pregnancy needs enough space for the baby, the amniotic fluid (liquor), and the placenta. At the start of pregnancy, the uterus is shaped like a pear. At 12 weeks, it becomes round (globular). From 12 to 38 weeks, it becomes oval-shaped. After 38 weeks, when the baby drops into the pelvis (lightening), it turns back to a round globular shape.
The Three Muscle Layers of the Myometrium
- Outer Longitudinal Layer: This layer starts in the front wall of the upper uterus, goes over the top (fundus), and down the back wall. When this muscle layer contracts and pulls back (retracts), it pushes the baby out during labor.
- Middle Oblique Layer: Here, muscles are arranged in a criss-cross way, looking like a "figure of 8" around the blood vessels. After the baby is born and the placenta separates, these muscles squeeze the blood vessels tight to stop bleeding and prevent Postpartum Haemorrhage (PPH). Because of this action, they are called living ligatures.
- Inner Circular Layer: This is the weakest of the three layers. The muscle fibers run straight across the uterus. They are well developed around the cervix, lower uterus, and fallopian tubes. They help the cervix to open (dilate) during labor.
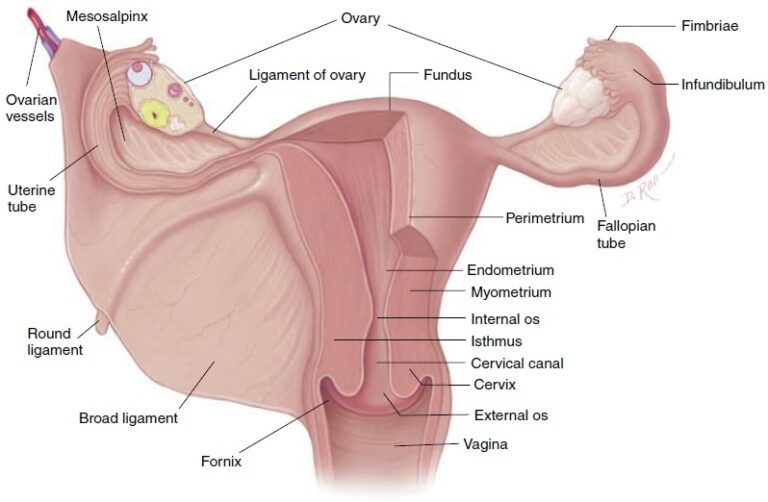
- 3. The Perimetrium: This is the outer layer of the peritoneum that covers most, but not all, of the uterus. It folds over the bladder in the front to form the utero-vesical pouch, and folds in the back to form the pouch of Douglas. After 12 weeks, the uterus grows so big it rises out of the pelvis and becomes an organ in the abdomen. It loses its forward-bending position and stands straight up, leaning slightly to the right side.
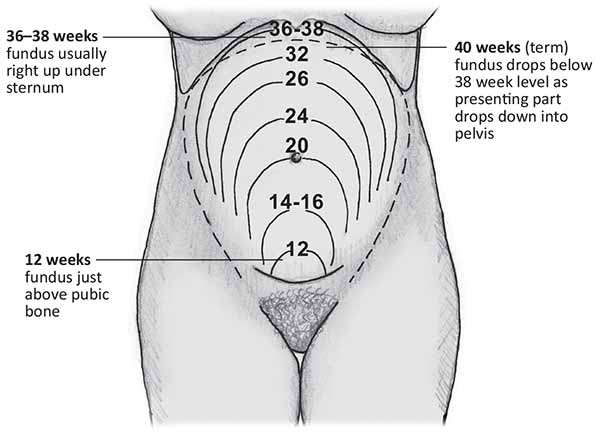
Clinical Observations of the Growing Uterus
As the pregnancy progresses, midwives check the size of the uterus (fundal height) to ensure the baby is growing well:
- At 12 weeks: The uterus comes out of the pelvis and stands straight. It can be felt just above the symphysis pubis (pubic bone) and is about the size of a grapefruit.
- At 16 weeks: The top of the uterus (fundus) becomes shaped like a dome. As it grows up, it twists slightly to the right side (dextrorotation) because the colon is on the left side of the pelvis. The uterus becomes more round.
- At 20 weeks: The fundus can be felt right at the level of the mother's umbilicus (belly button).
- At 30 weeks: The fundus is halfway between the umbilicus and the xiphisternum (the bottom tip of the breastbone). The large uterus pushes the mother's intestines to the sides and upwards. If the mother lies flat on her back, the heavy uterus falls back against her spine and major blood vessels.
- At 36 weeks: The enlarged uterus fills the entire abdominal space. The fundus touches the very tip of the xiphoid cartilage at the ribcage.
- At 38 weeks: Between 38 and 40 weeks, the lower part of the uterus becomes smooth and soft. The uterus looks rounder, and the fundal height actually drops lower. This drop happens because the baby's head enters the pelvis, a process called lightening.
Changes in Other Reproductive Organs
- Blood Supply: The blood vessels in the uterus get much wider, and new blood vessels form because of Oestrogen. Blood flowing to the uterus and ovaries increases to an amazing 750ml per minute at the end of pregnancy to feed the hard-working placenta.
- Fallopian Tubes: They are stretched out on both sides of the big uterus and get a rich blood supply. The end connected to the uterus closes, but the finger-like ends (fimbriae) stay open.
- The Isthmus: It becomes very soft and stretches out from just 7mm to 23mm long. This stretched part becomes the lower uterine segment in late pregnancy.
- The Ovaries: The Follicle-Stimulating Hormone (FSH) stops working because of high levels of estrogen and progesterone. This stops ovulation and menstrual periods. Both ovaries get bigger due to extra blood flow, and they are lifted out of the pelvis. The corpus luteum grows big in early pregnancy (sometimes forming a harmless cyst) to produce progesterone, which protects the early pregnancy until 10-12 weeks when the placenta takes over. After that, it shrinks.
- The Cervix: It stays tightly closed to protect the baby from infections and hold the baby inside when the mother stands up. It grows slightly and becomes very soft due to extra blood and relaxing hormones. The glands secrete a very thick mucus that blocks the cervical canal, called the operculum (mucus plug). Near labor, the cervix becomes part of the lower uterine segment (effacement) and opens slightly. A soft, slightly open cervix is called a "ripe cervix."
- The Vagina: The muscles grow thicker, and the vagina becomes bigger and very elastic so it can stretch during birth. It produces more normal white discharge called leucorrhea. The cells have a lot of glycogen (sugar), which interacts with normal bacteria (Doderlein’s bacillus) to make the vagina very acidic. This acid kills bad bacteria but makes the mother more likely to get yeast infections like Candida albicans. The extra blood makes the vagina look purple or violet.
- The Vulva: It also appears bluish in color because of the heavy blood flow and pelvic congestion.
Breast Changes
- In early pregnancy, breasts feel full, heavy, or tingle, and they grow bigger as pregnancy continues.
- The nipples stick out more easily (become more erectile).
- The dark circle around the nipple (areola) becomes much darker and wider.
- Small oil glands on the areola grow big and look like small bumps. These are called Montgomery’s tubercles. They produce oil (sebum) to keep the nipple soft and lubricated for breastfeeding.
- Blue blood vessels become very easy to see on the skin of the breasts because of the increased blood flow.
- A clear or yellowish sticky fluid called colostrum can sometimes be squeezed from the nipples after the first 3 months (1st trimester).
3. Changes in the Cardiovascular System (Heart and Blood)
The Heart and Blood Pressure
- The Heart: Because it has to work so hard, the heart muscle grows slightly bigger (hypertrophies), especially the left side. The growing uterus pushes the heart upwards and to the left side of the chest. Heart sounds change, and harmless heart murmurs are very common. The amount of blood the heart pumps (cardiac output) increases by 40%. The heart beats faster by an average of 15 extra beats every minute.
- Blood Pressure (BP): In the first 3 months, BP stays normal. In the second trimester, BP actually drops because the hormone progesterone causes blood vessels to relax and open wide (vasodilation). It is at its lowest between 16 and 20 weeks, which can cause the mother to feel dizzy or faint. Near the end of pregnancy, BP goes back to normal levels.
⚠️ Clinical Alert: Supine Hypotensive Syndrome
A pregnant woman should not lie flat on her back (supine position). The heavy baby and uterus will press down on the large vein in the back (inferior vena cava). This traps the blood, stopping it from returning to the heart. This causes a sudden, dangerous drop in blood pressure, making the mother faint. It also causes swelling (oedema) in the legs, swollen leg veins (varicose veins), and swollen veins in the anus (hemorrhoids). Always encourage the mother to sleep on her side.
Blood Volume and Composition
- Blood Flow: Much more blood flows to the uterus, kidneys, breasts, and skin. Blood flow to the liver and brain stays the same. Blood flow to the kidneys goes up by 70-80%.
- Total Blood Volume: The total amount of blood in the mother's body increases a lot, usually by 35% to 45% above normal. She needs this huge amount of extra blood to:
- Give the placenta enough blood to feed the baby.
- Meet the extra energy needs of the growing baby.
- Ensure the kidneys and other organs get enough oxygen.
- Protect the mother from danger when she loses blood during delivery.
- Physiological Anaemia: The liquid part of the blood (plasma) increases by 40%, but the red blood cells only increase by 20%. Because there is so much more water than red cells, the blood becomes diluted. This is perfectly normal and is called physiological haemodilution. The acceptable Hemoglobin (Hb) level during pregnancy is 11-12g/dl.
- Iron Metabolism: The mother needs a massive 1000mg of iron. She needs 500mg to make extra red blood cells, 300mg to give to the baby, and 200mg to replace iron naturally lost every day. Because the body only absorbs 20% of the iron she eats, she must take iron tablets. The goal of iron tablets is to prevent true anemia, not just to raise her Hb levels artificially.
- Clotting Factors: Proteins in the blood that cause clotting (Fibrinogen and factors 7, 8, 9, and 10) increase heavily. Because of this, her blood clots much faster (clotting time drops from 12 minutes to 8 minutes). This is the body's smart way of preventing heavy bleeding (PPH) when the placenta tears away after birth.
- White Blood Cells: These cells fight infection and are slightly increased during pregnancy (from normal levels up to 10,500/mm) and can jump up to 16,000/mm during labor. This keeps her immune system active.
4. Systemic Changes (Breathing, Urine, and Digestion)
Respiratory System (Breathing)
- The body burns more energy at rest (basal metabolism increases). The mother breathes in slightly more air with every breath because the baby, the mother's working heart, and her lungs need more oxygen.
- In late pregnancy, the mother's ribcage opens up wider (flares out). The huge uterus pushes the breathing muscle (diaphragm) high into the chest, squeezing the bottom of the lungs. This can make the mother feel slightly short of breath.
Urinary System
- Blood flow to the kidneys and the speed at which they filter waste (glomerular filtration rate) increase by 50%.
- Because of the large uterus pressing on the bladder, the mother has to urinate very often (frequency) in early and late pregnancy.
- The tubes connecting the kidneys to the bladder (ureters) become long and bent (kinked) because of the relaxing effects of progesterone. This causes urine to get trapped or move slowly, making pregnant women very easy targets for Urinary Tract Infections (UTIs).
Gastrointestinal System (Digestion)
- Gums: They become swollen with fluid, soft, spongy, and can bleed easily when brushing teeth.
- Ptyalism: This is a condition where the mother produces too much saliva.
- Nausea and Vomiting: This is very common, affecting 70% of pregnant women, especially early in the morning.
- Taste: Foods might taste different, sometimes leaving a metallic taste in the mouth.
- Pica: A strange craving to eat things that are not food, like soil, clay, or wall plaster.
- Appetite: Most women feel much hungrier.
- Heartburn: As the uterus grows, it leaves less space for the stomach. Stomach acid gets pushed up into the chest, causing a burning pain.
- Constipation: Progesterone relaxes the bowel muscles, so food moves very slowly through the intestines, causing hard stools.
5. Metabolism, Weight Gain & Muscles/Bones
Weight Gain in Pregnancy
The mother's metabolism speeds up to provide plenty of nutrients to the baby. Because of this, she steadily gains weight, which is a good sign that the baby is growing healthy. The average weight gain for a normal pregnancy is about 12.5 kg.
How the weight is gained:
- In the first 20 weeks: Gains about 4 kg (0.2 kg per week).
- In the last 20 weeks: Gains about 8.5 kg (0.4 kg per week).
| Body Part | Maternal Weight Gain (kg) | Fetal Weight Gain (kg) | Total Weight Gain (kg) |
|---|---|---|---|
| Uterus | 1.0 | - | 1.0 |
| Breasts | 0.4 | - | 0.4 |
| Fat Stores | 3.5 | - | 3.5 |
| Blood Volume | 1.5 | - | 1.5 |
| Extracellular Fluid | 1.5 | - | 1.5 |
| Fetus (Baby) | - | 3.4 | 3.4 |
| Placenta | - | 0.6 | 0.6 |
| Amniotic Fluid | - | 0.6 | 0.6 |
| Total | 7.9 | 4.6 | 12.5 |
Important Factors That Influence Weight Gain
Many details affect exactly how much weight a mother will put on during her pregnancy. A midwife must monitor these closely:
- Maternal Oedema (Swelling): Edema, or swelling, can directly affect weight gain. It involves the gathering and trapping of extra body fluid in the tissues (especially in the legs and feet). This extra water weight adds pounds on the scale.
- Maternal Metabolic Rate: The speed at which the mother's body burns energy (metabolic rate) impacts weight gain. A mother with a very fast, high metabolic rate uses up more energy quickly, which may result in her gaining less weight overall.
- Dietary Intake: The amount (quantity) and the healthiness (quality) of the food the mother eats play a massive role. Eating a well-balanced, highly nutritious diet ensures that the weight she gains is healthy and beneficial for the baby.
- Vomiting or Diarrhea: If a mother suffers from frequent vomiting (like in severe morning sickness) or diarrhea, it can cause weight loss or stop her from gaining the weight she needs. This happens because the body loses water and fails to absorb important calories and nutrients from food.
- Amount of Amniotic Fluid: The volume of the water surrounding the baby (amniotic fluid) is heavy. If the mother has an unusually large amount of fluid (a condition called polyhydramnios), it will lead to a much higher number on the weight scale.
- Size of the Fetus: Simply put, larger babies weigh more. A fast-growing or naturally large baby will cause the mother's total pregnancy weight gain to increase.
- Maternal Physical Activity Level: How much a mother exercises or moves around during the day impacts her weight. A mother who maintains regular physical activity burns more calories, which helps her keep her weight gain in a healthy range.
- Maternal Genetics: Family history and genes also play a part. Genetic factors can make a woman naturally more likely to gain extra weight quickly or hold onto weight longer during her pregnancy.
Musculo-Skeletal System (Muscles and Bones)
The hormones Progesterone and Relaxin cause the ligaments, joints, and muscles in the pelvis to soften and relax. This relaxation allows the pelvic bones (like the symphysis pubis in the front and the sacroiliac joints in the back) to spread out slightly. This increases the capacity of the pelvis, giving the baby enough room to pass through during labor (this process is known as a "give"). Because the joints are loose and the heavy uterus pulls the body forward, the mother's balance changes, leading to the typical "waddling" pregnant walk (gait).
6. Skin Changes
The pituitary gland produces more melanin-stimulating hormone, which causes different parts of the pregnant woman's skin to become dark (pigmentation). This usually starts in the 2nd month and lasts until birth. The areas most affected are the nipples, the middle line of the stomach, the perineum, and the armpits. This happens because the pigment cells become highly sensitive.
- Linea Nigra: This is a dark, visible line that runs straight down the middle of the belly, from the umbilicus to the pubic bone (and sometimes up to the chest). It is caused by hormones and will fade away after delivery, though it may never completely vanish.
- Chloasma (Mask of Pregnancy): This is the brownish darkening of the skin on the mother's face, usually over the forehead, nose, and cheeks. It gives the skin a bronze look, especially in women with dark complexions.
- Striae Gravidarum: These are the common stretch marks that appear on the skin of the growing belly, breasts, and thighs as the skin stretches rapidly.
- Sweat Glands: The sweat glands all over the body become much more active. This causes the pregnant woman to sweat more heavily. Also, because she has extra blood flowing and her base body temperature rises by 0.5 degrees, the mother will frequently feel hot.
❓ Quick Review
Why do pregnant women often complain of dizziness when lying flat on their back?
- Answer: When lying flat, the heavy uterus presses against the large inferior vena cava vein in the back. This blocks the blood from returning safely to the heart, dropping her blood pressure and causing dizziness (Supine Hypotensive Syndrome).

THANKS it’s simple to understand your work