

POSITIONING OF A CASUALTY:
A casualty is nursed in different positions in different situations. The commonly used positions are;
- Recovery position
- Prone position
- Fowler’s position/ sit up position
- Dorsal recumbent position.
- Positioning in shock.
RECOVERY POSITION:
This is used in unconscious patients/ casualties if breathing and has heart beat should be nursed in recovery position.
ADVANTAGES:
- It maintains open air way.
- The tongue cannot fall to the back of the throat.
- Head and neck will remain in the extended position so that the air passage is widened and that any vomiting or other fluid in the casualty’s mouth will drain freely.
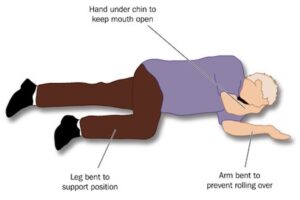
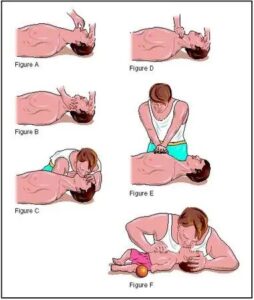
The recovery position is as follows:
- Place the body in the prone position.
- Turn the head down to the one side. No pillows should be used under the head.
- Pull up the leg and the arm on the side to which the head is facing.
- Pull up the chin.
- Stretch other arm out as shown.
- His clothes should be loosened at the neck and waist and any artificial tooth should be removed.
NOTE: Recovery position cannot be used in:
- When there are fractures to the upper or lower body.
- When the casualty is lying in a confined space or if it is not possible to bend the limbs.
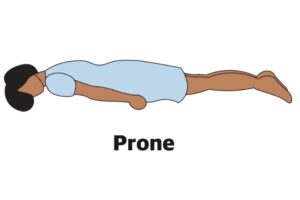
- PRONE POSITION
A patient is placed on his abdominal with head turned to one side. A pillow is placed under the head and hand’s kept on sides. This position is used for patients with burns of the back.
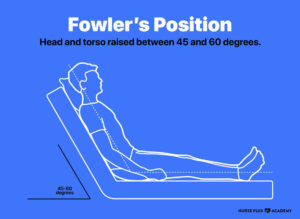
- FOWLER’S POSITION/ SIT UP POSITION
When a patient is having difficulty in breathing, this position is used. The patient is kept in a sitting position with the help of 3 or 4 pillows.
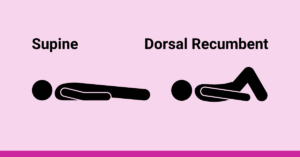
4. DORSAL RECUMBENT POSITION
The patient is kept on his back. A pillow is placed under the head. It is used for examination of the patient. This position without pillow is used in case of fracture of the spine and also to give CPR (cardio pulmonary resuscitation)
5. POSITIONING IN SHOCK.
Lay the casualty on the back turn head to one side. Raise the legs with two pillows to improve blood supply to the heart. If the victim has fracture on the lower limbs, it should not be elevated unless they are well splinted.

RESUSCITATION (BASIC LIFE SUPPORT)
Basic life support is an emergency life saving procedure that consists of recognizing and correcting failure of the respiratory and the cardio vascular system.
Basic life support comprises of ABC steps which concern the Airway, Breathing, and Circulation respectively.
For any one’s life to continue, the body needs adequate supply of oxygen to enter the lungs and transferred to all cells of the body through the blood stream. The most critical organ that should not fall short of Oxygen is the brain since it’s the master controller of all body functions.
Brain damage is possible if the brain is deprived of Oxygen for 4-6 minutes.
NOTE: Once you have started basic life support, do not interrupt it for more than 5 seconds for any reason accept it’s necessary to move the patient. Even in that interruption should not exceeds 7 seconds each.
THE RESUSCITATION SEQUENCE
- 1. CHECKING RESPONSE:
- On discovering a collapse casualty, you should first establish whether he/she is conscious by asking simple questions like, what has happened or command the patient to do something e.g. ‘’open your eye’’.
- Speak loudly and clearly close to the casualty’s ears. If the casualty does not respond, try to shake his shoulders gently as you speak to him/her (fully unconscious casualty will make no response at all).
- The casualty may respond to pain, so you can gently pitch his/her skin.
- A casualty who is partially conscious makes unnecessary movements on pitching.
NOTE: Quick assessment can be done using the ‘’AVPU’’ code.
A – Alert
V – Response to voice
P – Response to pain
U – Unresponsive.
CHECK POINTS
- Eyes
- Speech
- Movement
HOW TO OPEN THE AIRWAY
- Place the person in are recumbent position (face up) on a hard surface.
- Place one hand on his fore head and gently tilt his head back. As you do this, the mouth will fall open slightly.
- Place the finger tips of your hand on the point of the casualty’s chin and lift the chin up.
- Check the casualty’s breathing.
HOW TO CHECK FOR BREATHING:
Keeping the air way open look, listen and feel for normal breath.
- Look for chest movements.
- Listen for sounds of breathing.
- Feel for breaths on your own cheek and see movement.
- Along her chest and abdomen.
Do this for not more than 10 seconds before deciding whether the casualty is breathing normally.
NOTE: If there is any doubt, act as if breathing is not normal.
IF THE CASUALTY IS BREATHING
- Check the casualty for any life threatening injuries e.g. severe bleeding and manage it as necessary
- Place the casualty in a recovery position.
- Call for emergency help e.g. call for the nearest ambulance services.
- Monitor and record vital signs for example, level of response, breathing as you wait for help to arrive.
IF THE CASUALTY IS NOT BREATHING
- Shout or ask for help (dial for an ambulance).
- Begin cardio- pulmonary resuscitation with chest compressions.
HOW TO GIVE CARDIO PULMONARY RESUSCITATION
- Kneel the casualty’s level with his chest.
- Place the heel of one hand on the center of the casualty’s chest.
- Place the heel of your other hand on top of the first hand and interlock your fingers making sure the fingers are kept off the ribs
- Leaning over the casualty with your arms straight, press down vertically on the breast bone. (Sternum) and depress the chest 5 – 6cm (2 – 2 1/2inch).
- Allow the chest to come back up fully before giving the next compression.
- Compress the chest 30 times at a rate of 100 – 120 compressions per minute. The time taken for compression and release should be about the same.
- Move the casualty’s head and make sure that the airway is still opened.
- Put one hand on his fore head and two fingers of the other hand under tip of his chain.
- Move the hand that was on the fore head down to pitch the soft part of the nose with the finger and the thumb.
- Allow the casualty’s mouth to fall open.
- Take a breath and place your lips around the casualty’s mouth making sure that you have made a good seal. Blow into the casualty’s mouth until the chest rises. A complete rescue breath should take one second. Adjust the head position if the chest doesn’t rise.
- Maintaining the head tilt and chin lift, take your mouth off the casualty’s mouth and look to see the chest fall. If the chest rises visibly as 61,000 and falls fully when you lift your mouth a way, you have given a rescue breath. Give a second rescue breath.
8. Continue the cycle of 30 chest compressions followed by two rescue breaths. This is done until emergency help arrives or another first aider takes over or until the casualty shows signs of regaining consciousness, such as coughing, opening eyes, speaking or moving purposely e.tc. It can also be until you are too exhausted to continue.
Some notice for anatomy are not opening
The best
Thanks
well done