
Antenatal Care & Pelvic Assessment
1. Aims of Antenatal Care
The primary goals of providing antenatal care are to ensure a safe pregnancy and a healthy outcome for both mother and baby. These aims include:
- To monitor the progress of the pregnancy in order to support maternal health and ensure normal fetal development.
- To prepare the mother for labor, lactation (producing breast milk), and the subsequent care of her newborn baby.
- To detect early and treat appropriately any high-risk conditions—whether medical or obstetrical—that could endanger the life of the mother and the baby.
How These Aims Are Achieved
A midwife achieves these goals through the following practical steps:
- Developing a strong partnership with the pregnant woman.
- Providing a holistic (complete) approach to the woman’s care that meets her individual and personal needs.
- Promoting awareness of public health issues for the woman and her family.
- Exchanging information with the woman and her family, enabling them to make informed and smart choices.
- Being an advocate for the woman and her family, supporting her right to choose care that is appropriate for her own needs and those of the family.
- Recognizing complications of pregnancy early and appropriately referring women to specialists within the multi-disciplinary healthcare team.
- Facilitating the woman to make an informed choice about methods of infant feeding, and giving appropriate and sensitive advice to support her decision.
- Facilitating the woman and her family in their preparations to meet the physical and financial demands of birth by making a clear birth plan.
- Offering continuous health education to prepare the couple for parenthood.
Activities Done in the Antenatal Clinic (ANC)
Every ANC clinic must offer a specific set of services to every mother:
- Registration: Officially recording the mother into the clinic system.
- Booking: Taking a comprehensive medical and social history.
- Special Tests and Investigations: Conducting blood and urine tests.
- Health Education: Teaching about healthy pregnancy habits.
- Immunization: Giving vaccines such as the Tetanus Toxoid.
- Treatment of Minor Disorders: Managing common pregnancy complaints like nausea or heartburn.
- Provision of Supplements: Giving essential vitamins like Iron and Folic Acid.
- Examination: Performing full physical and abdominal checks.
- Orientation of Mothers: Showing them around the maternity unit.
- Formulating a Birth Plan: Preparing for the day of delivery.
- Counseling: Offering emotional and psychological support.
- Referral of Cases: Sending complicated or high-risk cases to better-equipped hospitals.
2. Initial Assessment (The Booking Visit)
The first day a mother comes to the clinic is called the "Booking Day." It is the most detailed visit.
Objectives for the Initial Assessment
- To assess the mother's level of health by taking a detailed history and to offer appropriate screening tests.
- To ascertain baseline data (starting measurements) of her blood pressure, urinalysis, uterine growth, and fetal development. This baseline is used as a standard for comparison as the pregnancy progresses.
- To identify risk factors by taking accurate details of her past and present obstetric, medical, family, and personal history.
- To provide an opportunity to discuss any fears or concerns the woman has.
- To give advice pertaining to pregnancy in order to maintain the health of the mother and the developing fetus.
- To build the foundation for a trusting relationship in which the woman and the midwife are partners in care.
- To make appropriate referrals when additional health care or support needs have been identified.
Comprehensive History Taking
The midwife must ask detailed questions across multiple categories to ensure nothing is missed.
Demographic Data
- Name, Age, Address, and Occupation.
- Next of Kin (NOK): Their relationship to the mother, occupation, and contact details.
- Level of Education (LOE), Tribe, and Religion.
- Nearest health facility and the exact distance from her home.
Social History and Habits
- Smoking: Cigarettes contain nicotine which constricts (narrows) blood vessels leading to placental insufficiency. This can result in fetal hypoxia (lack of oxygen for the baby), small for dates babies, and abortions. The woman should be advised to reduce the number of sticks gradually to avoid withdrawal syndrome.
- Alcohol: Drinking alcohol carries a risk of trauma (accidents) which can result in abortion or placenta abruption. It also causes a loss of appetite leading to maternal malnutrition and small for dates babies.
- Marital Status: Is she married or single? Find out the number of years spent in the marriage and try to find out if she is happy and safe at home.
Home Environment
- House: Is it rented or her own? Note the number of rooms and the total number of occupants to check for overcrowding.
- Environmental Hygiene: How clean is the home surrounding?
- Resources: What is her primary source of water and food?
Family History
- The health status of the woman’s parents and her siblings. (If they are deceased, note the exact cause of death).
- Familial diseases (diseases that run in the family) for example, a history of cancer, diabetes, cardiac (heart) diseases, allergies, etc.
- Other serious illnesses in the family like mental illnesses or severe complications with pregnancy.
- History of multiple pregnancies (twins, triplets) in the family line.
Past Surgical and Medical History
- Past Surgical History: History of accidents involving the spine, pelvis, and lower limbs which would reduce the pelvic diameters. History of major operations like Caesarean Section (C/S) and pelvic operations. History of blood transfusion (which carries a risk of exposure to HIV/AIDS and iso-immunization).
- Past Medical History: Medical conditions that may complicate or be complicated by pregnancy, labor, and puerperium (e.g., sickle cell disease, Diabetes Mellitus, Hypertension). Childhood illnesses like rickets or poliomyelitis which can reduce pelvic diameters, hence leading to a contracted pelvis. Infectious diseases like TB and Hepatitis B. Sexually Transmitted Infections like syphilis and gonorrhea.
Gynecological and Menstrual History
- Gynecological Conditions: History of abortions, ectopic pregnancy, fibroids, etc.
- Gynecological Operations: Previous surgeries like myomectomy (removing fibroids), D and C (Dilation and Curettage), or evacuation of the uterus.
- Menstrual History: Menarche (when periods first started), length of periods, interval between periods, and amount of blood flow. Any history of Dysfunctional Uterine Bleeding (DUB) or pre-menstrual spotting.
- Family Planning: Any method of family planning ever used, any complaint she had about it, and the reason for stopping it.
Past Obstetrical History
- Previous Pregnancies: Ask about any abnormalities such as abortions, stillbirths, living children, their general health status, and their immunization status. Ask for the interval between pregnancies, the length of gestation, birth weight, fetal outcome, length of labor, presentation (how the baby came out), and type of delivery. Ask about any prenatal and postnatal complications, and if the previous babies were breastfed and for how long.
- Labor History: Ask about any operations, induction of labor, assisted delivery (vacuum/forceps), and Postpartum Hemorrhage (PPH).
- Puerperium (Postnatal) History: Check if her recovery was normal, or if she had any history of sepsis (severe infection) or PPH.
Present Obstetric History
- Gravidity: Total number of pregnancies.
- Parity: Number of deliveries past 28 weeks.
- LMNP: Last Normal Menstrual Period.
- WOA (Weeks of Amenorrhea): How many weeks she has gone without her period (gestational age).
📅 Calculating the Expected Date of Delivery (EDD)
The EDD is calculated by adding 9 calendar months and 7 days to the date of the first day of the woman’s last menstrual period. This is known as Naegele’s Rule.
This method assumes that:
- The woman takes regular note of the regularity and length of time between her periods.
- Conception occurred exactly 14 days after the first day of the last period (true if the woman has a regular 28-day cycle).
- The last period of bleeding was true menstruation (because sometimes early embryo implantation can cause slight bleeding).
- She has not been taking contraceptive pills, as break-through bleeding and lack of ovulation (anovulation) caused by pills can impact the accuracy of the LNMP.
Present Health Status
Finally, the midwife must check how the mother's body is functioning right now:
- Appetite: It is important to know because a poor appetite leads directly to malnutrition and anemia.
- Sleep: Find out if the mother sleeps well. If not, find out the cause, which could be due to worries, insects in bed, physical pain, or signs of illness.
- Micturition (Urination): It’s good to know whether the woman passes urine well because Urinary Tract Infections (UTI) are common in pregnancy due to the stagnation of urine in dilated and kinked ureters. In case of increased frequency without pain, the mother is counseled in relation to the normal physiology of pregnancy.
- Bowel Action: As constipation is very common in pregnancy, the mother is reassured and advised to take plenty of fluids and roughages (fiber-rich foods).
NB: Always conclude the history by asking the mother if she has anything else she would like to tell you.
3. Investigations and Clinical Tests
On the first day, every single pregnant woman should receive the following laboratory investigations to ensure her safety.
| Test / Investigation | Reason / Clinical Interpretation |
|---|---|
| Urinalysis | Tested for Albumen (indicative of Pre-eclampsia/PET), Acetone (indicative of dehydration), and Sugars (indicative of diabetes). |
| RPR / VDRL | Done routinely to test for and exclude Syphilis. |
| HIV Screening | Done to ensure the Elimination of Mother-to-Child Transmission (EMTCT) of HIV. |
| Blood Grouping | Done to know her blood type in case of an emergency requiring blood transfusion. |
| Hb Level (Hemoglobin) | It should be done on the booking day, then at 32-34 weeks, and lastly at 36 weeks to rule out anemia. |
| Coombs Test | It is done to detect harmful antibodies circulating in the mother's blood. |
Clinical Tests Done in the Clinic
- Weight: This is taken on every visit to ANC. The mother is expected to gain about 12.5kg during the whole pregnancy (4kg in the first 20 weeks and 8.5kg in the last 20 weeks). Excessive weight gain could be due to twins, a very big baby, or excess amniotic fluid (polyhydramnios). Failure to gain weight could be due to poor fetal growth.
- Height: It’s done on the booking visit, or in labor if the mother has not been attending ANC. The normal height should range between 152-170cm. A height below 150cm indicates a small pelvis, and a height above 170cm indicates a narrow pelvis.
- Shoe Size: Normal shoe size ranges between 5 and 8. If the shoe size is below 5, it strongly indicates a small pelvis.
- Blood Pressure (BP): This is done on every visit to ANC. The BP of a pregnant mother normal ranges from 90/60 to 140/90 mmHg. A raised BP is a danger sign and may be due to PET and eclampsia. Any rise of 30 mmHg (systolic) and 15-20 mmHg (diastolic) from what has been considered normal is dangerous, and the mother’s urine should be tested for proteins immediately. The mother is asked how she feels generally, especially her sight (checking for blurred vision), and then referred to the doctor.
4. Full Physical Examination
This includes a full head-to-toe review of the physical systems to ascertain the woman’s general health. The breasts, pelvis, and abdomen receive particular attention. The examination is carried out systematically beginning with the head and ending with the pelvis and abdomen.
- General Appearance: Observe her body type, weight, energy level, grooming (cleanliness), and posture. This is noted when the mother is entering the room or when she is sitting.
- Head: Check the scalp, check the hair (whether treated), and check the hair pattern distribution.
- Eyes: Look at the conjunctiva (inner eyelids) to check for anemia. Look at the sclera (white of the eyes) to check for jaundice. Ask about her vision and look for abnormal eye discharge.
- Nose: Check her sense of smell. Look for bleeding, obstruction, abnormal growths, and discharge.
- Oral Cavity: Check for toothache, check dentures, and observe the state of her lips. Ask about chewing or swallowing problems. Check the tongue and gums for paleness (anemia), and ask about her sense of taste.
- Ears: Check for any discharges or any hearing loss.
- Neck: Check neck movement. Palpate for swellings or enlarged salivary glands (parotid, sub-mandibular, sublingual), the thyroid gland, and lymph nodes (superficial cervical, deep cervical glands, and sub-clavicles). Palpate and observe the jugular veins and pulsation of the thyroid gland. Swelling of the thyroid gland may be due to iodine insufficiency, though during pregnancy there is a slight enlargement of the glands which may be due to a chronic cough. Extended jugular veins may be due to cardiac problems or anemia.
- Upper Limbs (Arms): There should be two arms with the same size and length. Check skin texture and look for muscle wasting. Examine the palms for their color. Check the fingernails to see if capillary refill is good, and look for oedema (swelling).
- Chest: Observe exactly how the mother is breathing to detect if she has problems with her respiratory system, like pneumonia.
Breast Examination
This is done carefully to promote proper breast feeding and exclude hidden abnormalities.
- Inspection (Looking): Observe for size, equality, shape, and pulling of the breasts. Look for signs of pregnancy and signs of abnormalities like changes in the skin (e.g., redness, orange-like discoloration). Look at the nipple for prominence, dimpling, retraction (pulled inwards), size, and whether it is flat or well protracted. Check for presence of scars, cracks, sores, and axillary extension (breast tissue under the arm).
- Palpation (Feeling): The breasts are examined by touch to find breast abnormalities and deep-seated masses.
- Back: Check for any fungal infections, surgical scars, and sacral oedema (swelling at the bottom of the spine, which may indicate dangerous PET or Eclampsia).
- Lower Limbs (Legs): Check size, muscle wasting, pain or stiffness of joints, pain in the calf muscles, oedema, varicose veins, extra digits (toes), any infections, and tibia/ankle oedema.
- Feet: Check hygiene, any fungal infections, and nails (check for venous return and color). Check the sole of the feet for cleanliness and color.
Perform a Homan’s Sign: Homans’s sign is often used in the diagnosis of deep venous thrombosis (DVT) of the leg. A positive Homans’s sign (which is calf pain when dorsiflexing/bending the foot upwards) is thought to be associated with the presence of dangerous blood clots (thrombosis). - Assess for maternal efforts.
- Vulva: Check for sores, warts, varicose veins, and abnormal discharges. Request the mother to cough while observing to check for stress incontinence or discharges.

5. Abdominal Examination
It is carried out from 24 weeks gestation to establish and affirm that the fetal growth is consistent with the gestational age during pregnancy.
Aims of Abdominal Examination
- To observe signs of pregnancy.
- To assess fetal size and growth.
- To assess fetal health by auscultating (listening to) the fetal heart.
- To detect any deviations from normal.
- To diagnose the location of fetal growth.
- To locate fetal parts.
Preparation and Procedure
- Ensure the mother has emptied her bladder within the last 30 minutes before the abdominal examination.
- Ensure privacy.
- The mother should be lying comfortably on a couch.
- Wash your hands, expose only the area of the abdomen that needs to be palpated, and cover the remainder of the woman to provide her privacy and protect her dignity.
The 3 Steps of Abdominal Examination
1. Inspection
Stand at the foot of the bed while the mother is on her back with her abdomen exposed from the xiphisternum up to the symphysis pubis. Look at the size, shape, operational scars, signs of pregnancy like darkening of the linea nigra below and above the umbilicus, fetal movements, and striae gravidarum (stretch marks).
2. Palpation (Leopold’s Maneuvers)
Stand at the right side of the mother. Ensure the pads of your fingers, and not the sharp tips, are used. Palpate as follows:
- Superficial palpation: For localized tenderness.
- Hypochondriac palpation: For enlarged organs under the ribs.
- Height of fundus estimation: To check growth.
- Pelvic palpation: To check for presentation (which part of the baby is entering the pelvis).
- Fundal palpation: To check for the lie (how the baby's spine aligns with the mother's).
- Lateral palpation: To check for position (where the baby's back is facing).
🤲 Pawlik’s Grip (Second Pelvic Grip)
During a deep pelvic palpation, a midwife grips the fetal head between the thumb and fingers of one hand to check for engagement (if the head has dropped into the pelvis). This specific maneuver is termed as Pawlik’s grip or the second pelvic grip.
3. Auscultation
This is the way of listening to the fetal heart to determine fetal wellbeing by use of a feto-stethoscope.
Abdominal Summary
Conclude your abdominal exam by noting: Height of fundus, Presentation, Lie, Position, and Fetal heart.
Case Summary
- Comment on all histories, general and abdominal examination.
- Give feedback to the mother.
- Give necessary advice.
- Provide the return date for the next clinic visit.
6. Ongoing Antenatal Care
Purpose of Ongoing Visits
- To continue to observe for maternal health and freedom from infections.
- To assess fetal wellbeing continuously.
- To ascertain that the fetus has adopted a lie and presentation that will allow a normal vaginal delivery.
- To offer an opportunity for the mother to express any fear or worries about pregnancy and labor.
- To ensure that the mother and family are confident enough to decide when true labor starts.
- To discuss any views about the conduct of labor and formulate a birth plan if required.
Risk Factors Arising During Pregnancy
Be highly alert if any of the following occur:
- Change in fetal movement pattern - increased or reduced movements.
- Hb (Hemoglobin) less than 10g/dl (severe anemia).
- Poor weight gain or sudden weight loss.
- Proteinuria (protein found in urine).
- BP (Blood pressure) above 140/90 mmHg.
- Uterus is either too large or too small for the calculated dates.
- Excess or decreased liquor (amniotic fluid).
- Malpresentation (baby is in the wrong position for birth).
- Any form of vaginal bleeding.
- Premature contractions.
- Vaginal infection.
- Head not engaged by 38 weeks in PGs (Primigravidas - first-time mothers).
On Each Visit, Do The Following:
- Review the clinic card and assess any past complaints.
- Take Blood Pressure, weight, and test urine.
- Carry out a general and abdominal examination.
- Give drugs (like iron, folic acid, anti-malarials) accordingly.
Indicators of Fetal Wellbeing
- Increased maternal weight in association with increasing uterine size.
- Fetal movements which follow a regular pattern throughout the pregnancy.
- Fetal heart rate is steady between 120-160 beats per minute.
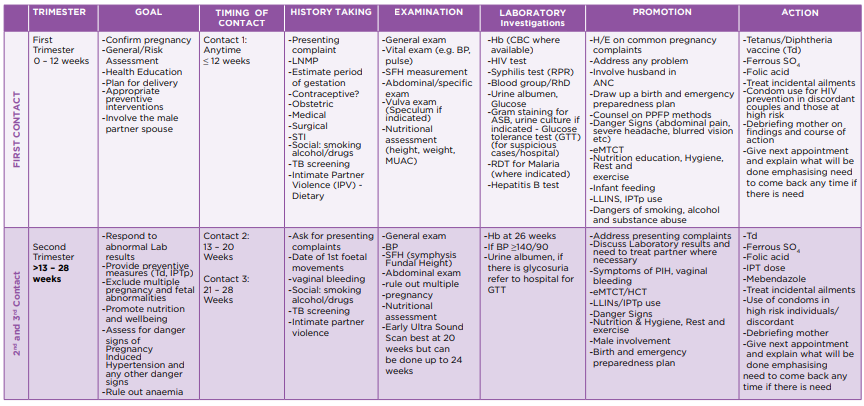
The MOH Goal Oriented ANC Protocol
Goals are different depending on the timing of the visit. A minimum of 8 Contacts are aimed for in an uncomplicated pregnancy. If a woman books later than in her first trimester, the preceding missed goals should be combined and attended to in the current visit. At all visits, the midwife must address any identified problems, check the BP, and measure the Symphysio-Fundal Height (SFH). Women must receive Hb, HIV testing, and Syphilis testing (RPR) routinely.
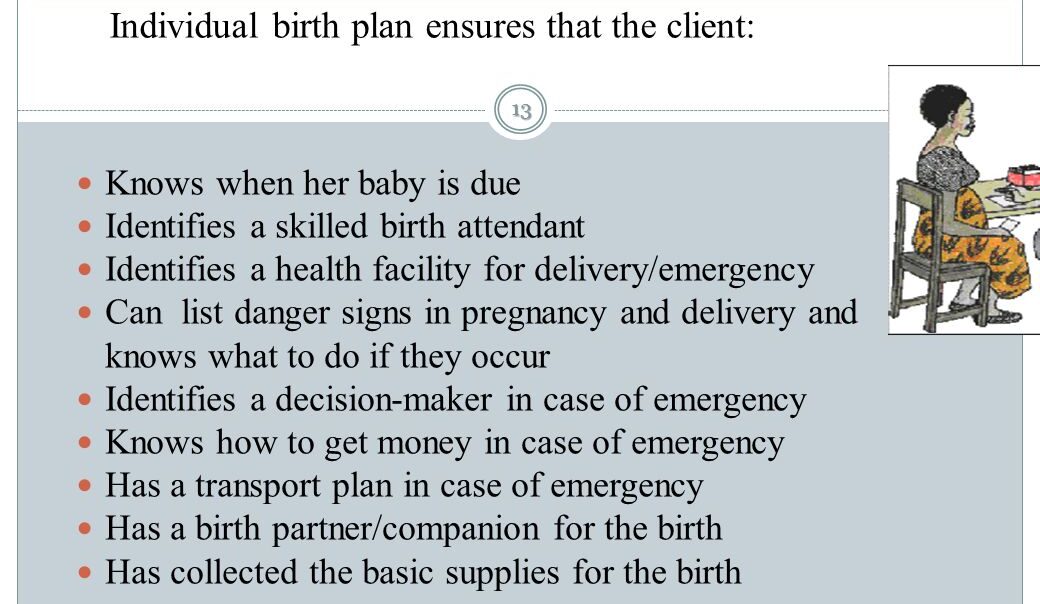
7. The Individual Birth Plan & Health Education
The Individual Birth Plan
A structured birth plan must be made to prepare the mother and her family. The plan includes:
- A birth place where there is a skilled birth attendant.
- Identifying someone to take care of the family in her absence.
- Knowing her EDD (Expected Date of Delivery).
- Her choice of a birth companion.
- Identifying a blood donor in case of emergency bleeding.
- Her choice of clothes for labor.
- Strategies for labor pain relief.
- Position for labor and childbirth.
- Place of delivery.
- Transportation to use and how it will be available.
- How to raise funds for transport and the cost of delivery.
- Family security and feeding provisions while she is away.
- Family planning goals for after the baby is born.
- Where to go after delivery.
- When her next appointment is.
NB: Involve the partner in the birth planning process. Teach the mother how to recognize the onset of true labor.
Health Education Topics
During the ANC visits, the midwife must continuously teach the mother about:
- Nutrition (eating a balanced diet).
- Sleep and resting.
- Sexual counseling.
- Hygiene.
- Daily activities.
- Healthy weight gain.
- Postnatal follow-up.
6. Immunization:
- TT (Tetanus Toxoid): Ensure the mother receives her Tetanus Toxoid injections to protect her and the newborn against tetanus.
Record and Interpret Findings
- After taking proper history, doing a thorough physical examination, and relevant investigations, record all findings clearly in the antenatal card.
- Interpret the findings accurately so as to identify any risk factors.
- Give care and management accordingly based on your findings.
- Give an appointment for the next visit accordingly.
📝 Assignment
Discuss the Goal Oriented Antenatal Protocol. Review the minimum 8 contacts, what is achieved at each contact, and how to combine goals for late bookings.
8. Pelvic Assessment
This is the estimation of the pelvic cavity so as to see whether it is adequate for that particular baby to pass through safely. OR, it is an examination done by a doctor or midwife on a pregnant woman at or after 36 weeks to see that both the mother and baby are out of danger at the time of delivery.
It is always done at 36 weeks because of the natural relaxation of the pelvic joints due to the Relaxin hormone.
Aims of Pelvic Assessment
- To rule out a poor obstetric history.
- To ensure normal delivery of the mother without any assistance (like vacuum or forceps).
- To rule out bone abnormalities like prominent ischial spines or a narrow sub-pubic arch.
- To reduce the infant and maternal mortality rate.
- To reduce injuries to both the mother and the fetus.
Pelvic assessment is done in 2 distinct ways: External Pelvic Assessment and Internal Pelvic Assessment.
A. External Pelvic Assessment (External Pelvimetry)
This is done on the 1st visit. It includes:
1. History Taking
- Age: A woman of the age of 18 years is expected to have a mature pelvis, but below 18 years, the bones are not fully ossified (hardened). A primigravida (PG) who is 35 years and above is expected to have a difficult delivery because the ligaments of the pelvis are already fused; therefore, the necessary "give" of the pelvis is impossible.
- Tribe: It’s important to know the tribe because different tribes have different types of pelvis structures. For example, the Bakiga and Banyankole have a large normal pelvis, but the Basoga and Baganda are at risk of having a contracted pelvis.
- Marital Status: It’s important to know the size of the husband because small women marrying giant men may carry big babies which can lead to CPD (Cephalopelvic Disproportion).
- Medical History: It’s important to know because some diseases like poliomyelitis may permanently affect the growth of the pelvic bones and muscles.
- Surgical History: Ask the mother if she has ever had any accident involving her spine, pelvis, and lower limbs.
- Past Obstetrical History: If the previous labor and delivery were completely normal, and if the baby weighed at least 3kg and over, she is expected to have an adequate pelvis. A history of instrumental delivery or C/S may give a strong suspicion of an inadequate pelvis.
2. Observations
- Gait: Always be alert on a woman who walks with a limp or who has muscle wasting of the legs. A poor gait means a deformed pelvis hence a reduced diameter. It often indicates congenital hip deformity.
- Height: The normal average height in women is between 152-170 cm. Height below 152cm may indicate a contracted pelvis, and if above 170cm, it indicates a narrow birth canal.
- Palms: Those with short palms usually indicate a small pelvis.
- Shoe Size: The normal shoe size is 4-8. A shoe size below 4 indicates a small pelvis.
- Stature: A woman of very small stature and a tiny waist is expected to have an inadequate pelvis.
3. Abdominal Examination: Engagement of the Fetal Head (Head Fitting)
NB: It’s no longer heavily practiced for fear of HIV transmission through aggressive handling.
Procedure for Head Fitting:
- Explain the procedure to the woman.
- The bladder should be completely emptied.
- The mother is relaxed flat on the bed with support on a pillow.
- The midwife with the right hand locates the symphysis pubis while the other hand is under the mother’s head.
- The mother takes a deep breath in and out.
- The baby's head is pushed downwards and inwards.
- The fingers of the right hand should feel if the largest transverse diameter of the fetal head is passing easily through the pelvic brim as the mother is supported to sit upright without relaxing her elbows.
- If the transverse diameter can be pushed through the pelvic brim, the top of the pelvis is adequate. This test is called head fitting.
NB: It’s incredibly important that from 36 weeks onwards, the abdomen is palpated to see if the head is engaged or can be made to engage.
B. Internal Pelvic Assessment (Digital Pelvimetry)
It’s done under strict aseptic (sterile) technique. The midwife must first clearly know the exact measurement of her own fingers.
Procedure:
- Explain the procedure thoroughly and ask the mother to empty her bladder and rectum.
- Prepare a Vaginal Examination (VE) tray and put it on the side of the bed.
- Screen the bed for absolute privacy.
- Ask the mother to lie on her back and carry out a routine abdominal examination first.
- The midwife measures the length of her working fingers.
- Position the mother in a dorsal position (knees bent, legs apart) and drape her to protect dignity.
- The right hand is gloved, and two fingers of the gloved hand are heavily lubricated, introduced, and passed high into the vagina. The following key pelvic areas are assessed:
Areas Assessed Internally
| Pelvic Structure | Assessment Detail |
|---|---|
| Sacral Promontory | An attempt is made to reach the sacro-promontory bone at the back by assessing the diagonal conjugate, which is normally 12-13cm deep. If the midwife's short fingers (less than 12-13cm) easily reach it, that directly shows it’s too prominent and the pelvis is small. |
| Hollow of the Sacrum | This is the curve of the lower back bone. It should be well-curved and smooth. It should not be too long; if it’s flat, the internal cavity is severely reduced and internal rotation of the fetal head will be very difficult. |
| Pelvic Walls | These side walls are felt, and they should be smooth and straight down (flat). If they converge (slant) downwards like a funnel, the mid-cavity is reduced. |
| Greater Sciatic Notches | These gaps should feel wide. If they are reduced or tight, internal rotation of the baby's head will be difficult. |
| Ischial Spines | These two side bones are palpated to see whether they are sharp or prominent. The distance between them is estimated to ensure the baby won't get stuck. |
| Sub-Pubic Arch | The front arch is measured and should not be less than 90 degrees. It should comfortably accommodate 2-3 fingers. A narrow sub-pubic arch reduces the anteroposterior (AP) diameter of the pelvic outlet, trapping the baby. |
| Inter-Tuberous Diameter | The distance between the 2 ischial tuberosities (sitting bones) can be assessed by inserting a closed fist between them externally; it should freely admit 4 knuckles. |
NB: After the assessment, record all your findings clearly and give prompt, honest feedback to the mother.

Thank you
this was so helpful, thanks
very vital and so helpful for learning
very vital and helpful to me a health tutor
Pingback: Introduction to Reproductive Health - Midwives Revision