
🤱 Breast Complications
DME 211: Mastitis & Abscess
- Engorgement, Mastitis, Breast Abscess
- Risk factors: Cracked nipples, poor latch, stasis
- Management: Antibiotics, continued breastfeeding, drainage
Breast complications are disorders affecting lactating breasts, ranging from benign engorgement to infectious mastitis and surgical abscess. They are LEADING CAUSES OF EARLY WEANING in Uganda.
Milk not removed effectively (poor latch, skipped feeds)
Incomplete emptying of breast
Long intervals between feeds (baby sleeping)
Key factor: Cracked nipples (portal of entry)
Stasis → Tender lump → Area red/hot
Systemic symptoms (fever) = Mastitis!
If untreated → Suppuration → Abscess!
DURATION: Days to weeks if unmanaged
Physiological: Painful overfilling of breasts with milk, usually occurs Day 3-5 postpartum when milk "comes in".
Pathological: Poor drainage leading to vascular congestion and edema.
- Poor latch/attachment
- Infrequent feeding (<8 feeds/24hrs)
- Overproduction of milk (hyperlactation)
- Abrupt weaning
- Mother-baby separation
- Tight bra/binding (compresses ducts)
Enlarged, heavy, painful breasts
Nipples flattened (hard to latch)
Generalized swelling (not localized lump)
Overfull, shiny skin
Redness (diffuse, mild)
General malaise (mild discomfort)
Elevated temp NOT present (no fever!)
Difficulty expressing milk
Bilateral often
Rapid onset (overnight)
Ends with proper drainage
Area tender but not hot
Systemic signs ABSENT
Time: Day 3-5 postpartum (classic)
Drain frequently (feed 8-12 times/24hrs)
Remove milk effectively (check latch)
Add warm compress before feeds (5 min)
Ice packs after feeds (reduce edema)
No bottles/pacifiers (increases stasis)
Breast massage (toward nipple)
Reverse pressure softening (push fluid back)
Express milk if baby can't latch (pump/hand)
Advise against tight bras
Support with pillows
Teach correct positioning
Cabbage leaves (cold) - traditional but effective!
Oxytocin (let-down reflex)
Mild analgesics (Paracetamol)
Patience (resolves in 24-48hrs with drainage)
Lactation consultant referral if persistent
Educate on normal course
Temperature spikes? → suspect mastitis!
- ❌ Stop breastfeeding (worsens stasis!)
- ❌ Bind breasts tightly (blocks ducts!)
- ❌ Delay feeds (milk builds up!)
- ❌ Give water/glucose to baby (reduces feed frequency!)
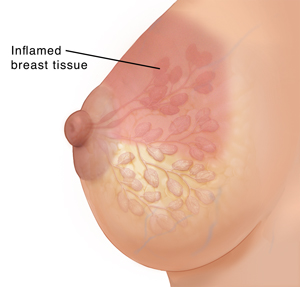
Inflammation of breast tissue, usually with bacterial infection, causing pain, swelling, warmth, and fever.
Incidence: 10-30% of lactating mothers in Uganda
Timing: Usually Week 2-6 postpartum (peak incidence)
- Lactational Mastitis: During breastfeeding (most common)
- Non-lactational Mastitis: Not related to breastfeeding (rare)
- Periductal Mastitis: Inflammatory condition near nipple
Cracked nipples (portal of entry for bacteria)
Restraint of milk flow (tight bra)
Abrupt changes in feeding schedule
Cloggged ducts (local stasis)
Key factor: Poor latch/attachment
Effective drainage absent (baby sleeping long)
Delayed feeds (scheduled vs demand)
Nipple trauma (pump misuse)
Immune suppression (fatigue, stress)
Previous episode (recurrence risk high)
Poor hygiene (handwashing)
Long intervals (night weaning)
Engorgement untreated
Smoking (reduces immunity)
Fever >38°C (systemic sign! Key differentiator!)
Erythema (localized redness, wedge-shaped)
Very painful breast (throbbing, tender)
Enlarged lymph nodes (axillary)
Rigors/chills
Lump (localized, palpable)
Uncertain borders (edematous area)
Maternal feels unwell (flu-like symptoms)
Pain increases with feeds (initially)
May have cracked nipple visible
Area hot to touch
Swollen segment of breast
Temperature difference (hot spot)
Illness duration: Rapid onset (24-48hrs)
Tenderness (severe)
Inflammatory signs dominate
Systemic antibiotics needed!
| Grade | Signs/Symptoms | Management |
|---|---|---|
| Mild | Local redness, pain, NO fever | Improve drainage, continue feeding |
| Moderate | Local signs + fever 37.5-38.5°C | Drainage + antibiotics |
| Severe | Fever >38.5°C, systemic illness | Antibiotics + analgesia + rest |
- Staphylococcus aureus (70-80% of cases) - from baby's nose/throat
- Streptococcus species (Strep. pyogenes, Strep. agalactiae)
- E. coli (less common, from gut flora)
- MRSA increasing in hospital settings
Localized collection of pus in breast tissue, resulting from untreated or inadequately treated mastitis.
Incidence: 3-11% of mastitis cases progress to abscess if untreated
Timing: Usually Week 3-8 postpartum (later than mastitis)
Fluctuation: KEY SIGN! Wave-like fluid feel
Localized swelling (discrete lump)
Ulceration of overlying skin (if severe)
Centally soft (edges indurated)
Tenderness (severe, localized)
Underlying cavity (pus present)
Antibiotics alone WON'T CURE
No improvement after 48hrs of antiobiotics
Temperature may be lower than mastitis (localized)
Area of redness (circumscribed)
Breast feels heavy
Systemic symptoms mild/moderate
Collections seen on ultrasound (if available)
Evolves from untreated mastitis
Surgical drainage required!
Suppuration (pus formation)
- Inspection: Localized swelling, erythema, skin may be shiny
- Palpation: FLUCTUANT mass, tender, warm
- Axilla: Tender lymph nodes often present
- Nipple: May have discharge (pus) when expressed
- Hypoechoic (dark) fluid-filled cavity
- Well-defined walls
- Septations if chronic/multiple loculi
- Useful to confirm diagnosis and locate depth

| Feature | Mastitis | Breast Abscess |
|---|---|---|
| Definition | Inflammation ± infection | Localized pus collection |
| Timing | Week 2-6 postpartum | Week 3-8 postpartum |
| Fever | HIGH (>38°C) | Low-grade or absent |
| Mass | Indurated (hard), diffuse | FLUCTUANT (fluid) |
| Pain | Diffuse, severe | Localized, severe |
| Skin | Erythematous, warm | Shiny, may ulcerate |
| Management | Drainage + antibiotics | INCISION & DRAINAGE + antibiotics |
| Breastfeeding | CONTINUE! From both breasts | CONTINUE! From unaffected breast + expressed milk from affected side after I&D |
| Hospitalization | Usually outpatient | Usually required for I&D |
| Duration | Resolves in 48-72hrs with Rx | Weeks to heal, needs daily dressing |
1. Improve drainage: Correct latch, frequent feeds
2. Manual expression: If baby can't latch
3. Comfort measures: Warm before, cold after feeds
4. Support: Emotional support key!
5. Follow-up: In 24 hours (if worsening → suspect mastitis)
Antibiotics: Start immediately!
Breastfeed CONTINUOUSLY! (even from affected side)
Treat pain: Paracetamol + Ibuprofen
Drainage: Improve emptying (massage, position changes)
Rest: Mother must rest (key to recovery!)
Analyze cause: Check latch, fix underlying issue
Increase fluids
Non-negotiable: Complete antibiotic course!
Review in 48hrs (should be improving)
Educate: If not better → risk of abscess
Support groups: La Leche League, peer counselors
Treat baby for oral thrush if present
1. REFER TO HOSPITAL: Must be drained surgically!
2. INCISION & DRAINAGE:
• Radial incision (spoke-like) to avoid ducts
• General anesthesia or local + sedation
• Break loculi (multiple pockets)
• Insert drain (gauze or rubber)
3. DAILY DRESSING: Wet-to-dry dressings
4. ANTIBIOTICS: 10-14 days (IV then oral)
5. CONTINUE BREASTFEEDING:
• From unaffected breast - continue directly
• From affected breast - express milk AFTER drainage and discard for 24hrs, then resume
• Express milk regularly to maintain supply
6. ANALGESIA: Strong pain relief needed
7. FOLLOW-UP: Daily until healed (2-4 weeks)
| Drug | Dose | Duration | Comments |
|---|---|---|---|
| Cloxacillin | 500mg QID | 10-14 days | Covers Staph aureus, safe in lactation |
| Amoxicillin-Clavulanate | 625mg TID | 10-14 days | Broad spectrum, excellent coverage |
| Erythromycin | 500mg QID | 10-14 days | If Penicillin allergic, safe in lactation |
| Cephalexin | 500mg QID | 10-14 days | Alternative, good safety profile |
| Metronidazole | 400mg TID | 7 days | Add if anaerobic infection suspected (IBD) |
- 48 hours no improvement: Consider MRSA, change to Clindamycin 300mg QID
- Worsening after 24hrs: Add gentamicin IV, refer for admission
- Ultrasound shows abscess: Switch to IV antibiotics (Cloxacillin + Gentamicin)
✓ Cloxacillin = Safe
✓ Amoxicillin-Clavulanate = Safe
✓ Erythromycin = Safe
✓ Cephalexin = Safe
✓ Metronidazole = Safe in lactation (some give after feeds)
✓ Gentamicin = Safe (minimal oral absorption)
⚠️ Avoid: Tetracyclines, Chloramphenicol, Ciprofloxacin (if possible)
A) Stop breastfeeding and apply cold compresses
B) Continue breastfeeding, start antibiotics, and improve drainage ⭐ CORRECT
C) Immediate incision and drainage
D) Bind the breast tightly to reduce swelling
• Continue breastfeeding from both breasts (1 mark)
• Improve drainage (massage, position changes) (1 mark)
• Start antibiotics (Cloxacillin 500mg QID for 10-14 days) (1 mark)
• Analgesia (Paracetamol + Ibuprofen) (1 mark)
• Rest, fluids, review in 48hrs (1 mark)
• If no improvement → consider abscess/refer (1 mark, bonus)
Diagnosis: Breast abscess (progression from mastitis) - 2 marks
Management:
1. Refer to hospital for incision and drainage - 2 marks
2. Continue antibiotics (may need IV) - 1 mark
3. Continue breastfeeding from unaffected breast - 1 mark
4. Express and discard milk from affected breast 24hrs post-I&D - 1 mark
5. Provide analgesia - 1 mark
6. Daily dressing and follow-up - 1 mark
7. Counsel that breastfeeding can continue after 24hrs - 1 mark
b) Fluctuation on palpation confirms the diagnosis of breast abscess.
c) Cloxacillin is safe to use in lactating mothers.
a) FALSE - Must continue breastfeeding! Drains infection.
b) TRUE - Fluctuation = fluid = pus = abscess
c) TRUE - Drug of choice, safe for baby
Risk factors: Cracked nipples, poor latch, stasis, missed feeds, tight bra, previous mastitis, fatigue (any 4)
Complications: Breast abscess, sepsis, chronic infection, early weaning, breast deformity, recurrent mastitis (any 4)
MARKING: 1 mark per correct answer
Day 3-5: ENGORGEMENT (physiological)
• Bilateral, no fever, diffuse swelling
• Manage with drainage + comfort measures
Week 2-6: MASTITIS (infection + inflammation)
• Unilateral, FEVER + LUMP
• Manage with ABT + DRAIN + REST
• NEVER STOP BREASTFEEDING!
Week 3-8: ABSCESS (pus collection)
• FLUCTUANT MASS, may have less fever
• Manage with I&D + ABT + CONTINUE FEEDING
• Refer to hospital for drainage!
- Continue breastfeeding: Even with mastitis/abscess
- Drainage is key: Empty breast frequently
- Antibiotics for mastitis: 10-14 days minimum
- Fluctuation = I&D: No antibiotics alone for abscess
- Support the mother: Emotional support prevents weaning
- ✓ Correct latch from birth
- ✓ Feed on demand (8-12 times/24hrs)
- ✓ Complete emptying each feed
- ✓ Treat cracked nipples promptly
- ✓ Avoid tight bras/binding
- ✓ Rest, nutrition, fluid support
- ✓ Early recognition and treatment