
DAY 8
📅 Nov 17 (Sun)
🦴 Female Pelvis & Varieties
DME 111: Obstetric Anatomy
- Bony Pelvis: Bones, Joints, Landmarks
- Pelvic Types (Gynecoid, Android, Anthropoid, Platypelloid)
- Pelvic Assessment: Clinical & Imaging
🦴 REMEMBER: Gynecoid = Ideal for birth (50% women). Android = Male-type, difficult!
📏 KEY POINT: Diagonal conjugate = 12.5cm important! Assess inlet size!
"Know the passage to predict the journey!"
"You formed my inward parts." - Psalm 139:13
1. THE BONY PELVIS - INTRODUCTION
📚 Definition:
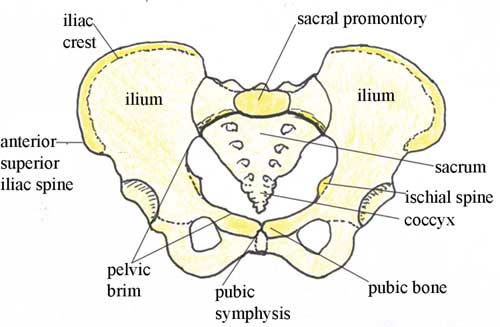
The pelvis is a bony ring formed by the sacrum, coccyx, and two innominate bones. It protects pelvic organs and forms the birth canal through which the fetus passes during delivery.
🌍 UGANDA CONTEXT: Pelvic size and shape directly affect labor outcomes! In rural areas with high rates of cephalopelvic disproportion (CPD), knowing pelvic assessment can save lives through early referral!
🦴 The Bones - The "3 Components":
🧠 MNEMONIC: "SACRUM COCCYX INNOMINATES"
Sacrum: 5 fused vertebrae, wedge-shaped, forms posterior wall
Articulates with ilium at sacroiliac joints
Curved shape creates pelvic cavity space
Ridges (promontory) important for measurement
Under the ilium in pelvic brim
Moves slightly during labor (tailbone flexes)
Coccyx: 3-5 fused vertebrae, triangular
Often moves backward during delivery
Can be fractured in difficult deliveries
Creates distance for fetal passage
Yields when sacrococcygeal joint flexes
X-ray shows position (if imaging used)
Innominate bones: Two hip bones (left & right)
Name means "no name" - each has 3 parts
Navigate the birth canal shape
Open and widen in pregnancy (hormones)
Meet at symphysis pubis anteriorly
Ilium, ischium, pubis fused at acetabulum
Narrow inlet/outlet affects labor
Angle of pubic arch varies by type
Transmits weight from spine to legs
Entire pelvis shape determines type
Shape assessed during ANC/pelvimetry
Sacrum: 5 fused vertebrae, wedge-shaped, forms posterior wall
Articulates with ilium at sacroiliac joints
Curved shape creates pelvic cavity space
Ridges (promontory) important for measurement
Under the ilium in pelvic brim
Moves slightly during labor (tailbone flexes)
Coccyx: 3-5 fused vertebrae, triangular
Often moves backward during delivery
Can be fractured in difficult deliveries
Creates distance for fetal passage
Yields when sacrococcygeal joint flexes
X-ray shows position (if imaging used)
Innominate bones: Two hip bones (left & right)
Name means "no name" - each has 3 parts
Navigate the birth canal shape
Open and widen in pregnancy (hormones)
Meet at symphysis pubis anteriorly
Ilium, ischium, pubis fused at acetabulum
Narrow inlet/outlet affects labor
Angle of pubic arch varies by type
Transmits weight from spine to legs
Entire pelvis shape determines type
Shape assessed during ANC/pelvimetry
🔍 The Innominate Bone - 3 Parts:
- Ilium: Upper fan-shaped part, iliac crest is landmark
- Ischium: Lower posterior part, ischial spine is KEY landmark
- Pubis: Anterior part, forms symphysis pubis joint
All three fuse at the acetabulum (hip socket) by adulthood
🔗 Pelvic Joints - The "3 Joints":
| Joint | Location | Function in Labor | Hormonal Effect |
|---|---|---|---|
| Symphysis Pubis | Anterior midline | Widens 2-3mm | Relaxin softens cartilage |
| Sacroiliac (2) | Posterolateral | Slight movement | Relaxin increases mobility |
| Sacrococcygeal | Posterior inferior | Coccyx flexes backward | Increases outlet diameter |
⚠️ EXAM CRITICAL: Hormones (relaxin, progesterone) soften pelvic joints in pregnancy. This increases mobility but can cause "pelvic girdle pain" - reassure mothers this is normal!
📏 Pelvic Planes - The "4 Planes":
📐 MNEMONIC: "INLET MID TRUE OUTLET PATHWAY"
Inlet (superior pelvic aperture): Brim of pelvis
• Boundaries: Sacral promontory, alae, arcuate line, pubic crest
• Shape varies by pelvic type
• KEY: Obstetric conjugate = shortest diameter (10cm)
Midplane (cavity): Smallest plane
• Boundaries: Midpoint of pubis, ischial spines, sacral hollow
• KEY: Interspinous diameter = 10cm (critical!)
• Ischial spines = landmark for descent (0 station)
Outlet (inferior pelvic aperture): Lower opening
• Boundaries: Pubic arch, ischial tuberosities, tip of coccyx
• KEY: Intertuberous diameter = 11cm
• Subpubic angle should be >85°
PATHWAY: The whole birth canal!
Inlet (superior pelvic aperture): Brim of pelvis
• Boundaries: Sacral promontory, alae, arcuate line, pubic crest
• Shape varies by pelvic type
• KEY: Obstetric conjugate = shortest diameter (10cm)
Midplane (cavity): Smallest plane
• Boundaries: Midpoint of pubis, ischial spines, sacral hollow
• KEY: Interspinous diameter = 10cm (critical!)
• Ischial spines = landmark for descent (0 station)
Outlet (inferior pelvic aperture): Lower opening
• Boundaries: Pubic arch, ischial tuberosities, tip of coccyx
• KEY: Intertuberous diameter = 11cm
• Subpubic angle should be >85°
PATHWAY: The whole birth canal!
💡 MASTER TIP: The midplane is the SMALLEST - often the point of obstruction! Ischial spines are the "bottleneck" - remember this!

2. PELVIC TYPES - THE "4 CLASSIFICATIONS"
📚 Caldwell-Moloy Classification:
Based on shape of pelvic inlet and architectural features. Determines obstetric outcome!
🧠 MNEMONIC: "GIRL-ANDROID-ANCIENT-PLATYPUS"
Gynecoid = Great for birth
Android = Awkward/difficult
Anthropoid = Ancient/ape-like
Platypelloid = Platypus-flat
Incidence:
• Gynecoid: 50% of women
• Android: 20-30%
• Anthropoid: 20-25%
• Platypelloid: 3-5% (RARE!)
Gynecoid = Great for birth
Android = Awkward/difficult
Anthropoid = Ancient/ape-like
Platypelloid = Platypus-flat
Incidence:
• Gynecoid: 50% of women
• Android: 20-30%
• Anthropoid: 20-25%
• Platypelloid: 3-5% (RARE!)
| Pelvic Type | Shape | Key Features | Obstetric Outcome | Incidence |
|---|---|---|---|---|
| Gynecoid | Round transverse | • Wide transverse diameterFAVORABLE | 50% | |
| Android | Heart-shaped | • Triangular inletUNFAVORABLE | 20-30% | |
| Anthropoid | Oval anteroposterior | • Long AP diameterMODERATE | 20-25% | |
| Platypelloid | Kidney-shaped/flat | • Short AP diameterPOOR | 3-5% |
📊 EXAM STRATEGY: In exams, describe pelvis by "shape, walls, spines, angle" - these 4 features distinguish types. They ask: "Describe features of android pelvis?"
🔍 Clinical Identification - External Clues:
👀 MNEMONIC: "LOOK AT THE MOTHER TO PREDICT PELVIS"
Gynecoid = Gently curved spine, wide hips
• Subpubic angle easily accommodates 2 fingers
• Intertuberous diameter >8.5cm
• Sacral curve normal
Android = Angular, masculine build
• Narrow hips, funnel-shaped pelvis
• Ischial spines prominent on exam
• Subpubic angle <2 fingers
Anthropoid = Ape-like, longer sacrum
• Narrow hips but deep pelvis
• AP diameter > transverse
Platypelloid = Plat, wide but shallow
• Wide hips, short sacrum
• AP diameter very short
Gynecoid = Gently curved spine, wide hips
• Subpubic angle easily accommodates 2 fingers
• Intertuberous diameter >8.5cm
• Sacral curve normal
Android = Angular, masculine build
• Narrow hips, funnel-shaped pelvis
• Ischial spines prominent on exam
• Subpubic angle <2 fingers
Anthropoid = Ape-like, longer sacrum
• Narrow hips but deep pelvis
• AP diameter > transverse
Platypelloid = Plat, wide but shallow
• Wide hips, short sacrum
• AP diameter very short
⚠️ EXAM CRITICAL: No pelvis is "pure" - most are MIXED TYPES! A woman may have gynecoid inlet but android outlet. Always assess all planes!
🎯 Implications for Labor:
- Gynecoid: CPD rare, normal progress expected
- Android: High risk of CPD, arrest of descent, need CS
- Anthropoid: Occipitoposterior position common, longer labor
- Platypelloid: Deep transverse arrest common, often requires CS
🌍 UGANDA CONTEXT: Many women with android pelvis present with prolonged labor in rural HC IIIs. Early pelvic assessment during ANC allows referral to HC IV/Hospital for trial of labor under monitoring. Don't attempt home delivery if android pelvis suspected!
3. PELVIC ASSESSMENT - CLINICAL & IMAGING
📏 Key Measurements - The "Critical 5 Diameters":
| Measurement | How to Measure | Normal Value | Clinical Significance |
|---|---|---|---|
| Diagonal Conjugate (DC) | Vaginal exam: sacral promontory to lower pubis | ≥12.5 cm | Inlet size, >11.5cm adequate |
| Obstetric Conjugate (OC) | Calculated: DC - 1.5-2cm | ≥10 cm | True inlet diameter, >10cm adequate |
| Interspinous Diameter | Vaginal exam: between ischial spines | ≥10 cm | Midplane, <10cm=midpelvic contraction |
| Intertuberous Diameter | External: between ischial tuberosities | ≥11 cm | Outlet size, <8cm=outlet contraction |
| Intercristal Diameter | External: between iliac crests | ≥28 cm | Predicts pelvic capacity |
💡 CRITICAL EXAM POINT: Diagonal conjugate is the ONLY inlet measurement you can do clinically! If DC <11.5cm, inlet contraction=HIGH RISK!
🩺 Clinical Pelvimetry - The "External 4":
✋ MNEMONIC: "HEAL PELVIS EXTERNALLY"
Height: <5 feet=risk of small pelvis
Evaluation of gait: Waddling gait = android pelvis?
Abdominal assessment: Fundal height, engagement
Look at body habitus: Android vs gynecoid build
Pubic angle: 2 fingers = adequate
External conjugate: PS to umbilicus (≥20cm)
Liaison: Feel iliac crest width
Value of thigh gap: Wide gap = favorable
Intertuberous diameter: External measurement
Sacral dimple position: Low dimple = short sacrum
Height: <5 feet=risk of small pelvis
Evaluation of gait: Waddling gait = android pelvis?
Abdominal assessment: Fundal height, engagement
Look at body habitus: Android vs gynecoid build
Pubic angle: 2 fingers = adequate
External conjugate: PS to umbilicus (≥20cm)
Liaison: Feel iliac crest width
Value of thigh gap: Wide gap = favorable
Intertuberous diameter: External measurement
Sacral dimple position: Low dimple = short sacrum
🔬 Internal Pelvimetry - The "Vaginal Exam 3":
- Diagonal Conjugate: Must be measured in early pregnancy (before engagement)
- Ischial Spines: Prominent? Favorable? Distance between?
- Sacral Curve: Straight (android) vs curved (gynecoid)
⚠️ CAUTION: Internal pelvimetry is CONTRAINDICATED in late pregnancy if placenta previa suspected! Always confirm placenta location first (ultrasound).
4. IMAGING PELVIMETRY - WHEN & HOW
📸 X-ray Pelvimetry - The "Old Gold Standard":
- Used: Only when CPD suspected, breech presentation, post-CS trial of labor
- Views: Lateral, AP, and inlet/outlet views
- Advantages: Accurate measurements, all diameters visible
- Disadvantages: Radiation exposure (teratogenic!), expensive, not routine
- Timing: After 36 weeks if absolutely necessary
🌍 UGANDA CONTEXT: X-ray pelvimetry is RARELY available in rural settings. Most facilities rely on clinical pelvimetry. If X-ray needed, refer to Regional Hospital. However, ultrasound is increasingly used!
🔍 CT & MRI Pelvimetry - The "Modern Methods":
| Method | Advantages | Disadvantages | Availability in Uganda |
|---|---|---|---|
| CT Scan | Very accurate, 3D reconstruction | High radiation dose, expensive | Only at Mulago, Mbarara |
| MRI | Excellent detail, no radiation | Very expensive, not tolerated in claustrophobia | Mulago, few private facilities |
| 3D Ultrasound | No radiation, good accuracy, portable | Operator-dependent, learning curve | Regional hospitals, some HC IVs |
💡 EXAM STRATEGY: Clinical pelvimetry is STANDARD in Uganda! Emphasize: "DC ≥12.5cm, interspinous ≥10cm, adequate external conjugate" = trial of labor suitable.
🎯 When to Suspect Pelvic Contraction:
⚠️ MNEMONIC: "CONTRACTED PELVIS SIGNS"
Cephalo-pelvic disproportion (CPD) history
Older primigravida (>35 years)
Nulliparous with android build
T Ricketts history (vitamin D deficiency)
Abnormal external measurements
Convex sacrum on exam
Trauma to pelvis (accident, fall)
Engagement doesn't occur by 38 weeks
Diagonal conjugate <11.5cm
Prolonged 1st stage with good contractions
Early decelerations (fetal distress)
Lack of descent despite pushing
Very prominent ischial spines
Interspinous <10cm (midplane contraction)
Severe molding with little descent
Cephalo-pelvic disproportion (CPD) history
Older primigravida (>35 years)
Nulliparous with android build
T Ricketts history (vitamin D deficiency)
Abnormal external measurements
Convex sacrum on exam
Trauma to pelvis (accident, fall)
Engagement doesn't occur by 38 weeks
Diagonal conjugate <11.5cm
Prolonged 1st stage with good contractions
Early decelerations (fetal distress)
Lack of descent despite pushing
Very prominent ischial spines
Interspinous <10cm (midplane contraction)
Severe molding with little descent
LIKELY EXAM QUESTIONS FOR DAY 8
1. FILL-IN-THE-BLANK (2 marks)
The ideal pelvic type for childbirth is ______ pelvis which occurs in approximately ______% of women.
ANSWER: Gynecoid, 50%
2. MULTIPLE CHOICE (3 marks)
A woman has a diagonal conjugate measurement of 11.0cm. This indicates:A) Adequate pelvic inlet
B) Borderline pelvic inlet
C) Contracted pelvic inlet ⭐ CORRECT
D) Cannot determine inlet size
EXPLANATION: DC <11.5cm indicates contracted inlet. Normal DC ≥12.5cm gives OC ≥10cm (adequate).
3. SHORT ANSWER (5 marks)
Differentiate between gynecoid and android pelvis based on shape and obstetric outcome.
ANSWER GUIDE:
Gynecoid: Round transverse, wide subpubic angle (90-100°), normal ischial spines, favorable outcome - 2.5 marks
Android: Heart-shaped, convergent walls, prominent spines, subpubic angle <90°, unfavorable (CPD risk) - 2.5 marks
Gynecoid: Round transverse, wide subpubic angle (90-100°), normal ischial spines, favorable outcome - 2.5 marks
Android: Heart-shaped, convergent walls, prominent spines, subpubic angle <90°, unfavorable (CPD risk) - 2.5 marks
4. PRACTICAL SCENARIO (10 marks)
During ANC, you examine a primigravida and find: diagonal conjugate 12.0cm, interspinous diameter 8.5cm, prominent ischial spines, subpubic angle <90°. What is your assessment and plan?
ANSWER:
Assessment: Mixed pelvic type - adequate inlet but contracted midplane/android features - 3 marks
Findings:
• DC 12.0cm = borderline inlet - 1 mark
• Interspinous 8.5cm = contracted (<10cm) - 1 mark
• Prominent spines = android - 1 mark
• Subpubic angle <90°=android - 1 mark
Plan:
• Refer for trial of labor at HC IV/Hospital - 2 marks
• Anticipate possible CPD/arrest - 1 mark
• Document findings in ANC card - 1 mark
Assessment: Mixed pelvic type - adequate inlet but contracted midplane/android features - 3 marks
Findings:
• DC 12.0cm = borderline inlet - 1 mark
• Interspinous 8.5cm = contracted (<10cm) - 1 mark
• Prominent spines = android - 1 mark
• Subpubic angle <90°=android - 1 mark
Plan:
• Refer for trial of labor at HC IV/Hospital - 2 marks
• Anticipate possible CPD/arrest - 1 mark
• Document findings in ANC card - 1 mark
5. TRUE/FALSE (2 marks each)
a) The interspinous diameter is the smallest pelvic plane and should be ≥10cm.b) Clinical pelvimetry should be performed in every woman at 38 weeks gestation.
c) Platypelloid pelvis is the most common pelvic type in African women.
ANSWERS:
a) TRUE - Midplane is smallest, <10cm is contracted
b) FALSE - Only indicated if risk factors/concerns; contraindicated if placenta previa
c) FALSE - Rarest type (3-5%), gynecoid is most common
a) TRUE - Midplane is smallest, <10cm is contracted
b) FALSE - Only indicated if risk factors/concerns; contraindicated if placenta previa
c) FALSE - Rarest type (3-5%), gynecoid is most common
6. LIST QUESTION (8 marks)
List four measurements obtained during clinical pelvic assessment and four features of an android pelvis.
ANSWER:
Measurements: Diagonal conjugate, interspinous diameter, intertuberous diameter, external conjugate, intercristal diameter (any 4)
Android Features: Heart-shaped inlet, convergent side walls, prominent ischial spines, subpubic angle <90°, narrow forepelvis, straight sacrum (any 4)
MARKING: 1 mark per correct answer
Measurements: Diagonal conjugate, interspinous diameter, intertuberous diameter, external conjugate, intercristal diameter (any 4)
Android Features: Heart-shaped inlet, convergent side walls, prominent ischial spines, subpubic angle <90°, narrow forepelvis, straight sacrum (any 4)
MARKING: 1 mark per correct answer
📊 STATISTICS: Pelvic anatomy appears in 85% of midwifery exams - often as "What pelvic type is favorable?" or "What does DC measure?" Master the types and measurements!
📚 DAY 8 SUMMARY: THE PELVIS DECODED
🎯 The 4 Pelvic Types at a Glance:
🦴 "GIRL-ANDROID-ANCIENT-PLATYPUS"
Gynecoid = Good (50%, round, favorable)
Android = Awful (20-30%, heart-shaped, CPD risk)
Anthropoid = Adequate (20-25%, long oval, OP common)
Platypelloid = Poor (3-5%, flat, deep arrest)
Gynecoid = Good (50%, round, favorable)
Android = Awful (20-30%, heart-shaped, CPD risk)
Anthropoid = Adequate (20-25%, long oval, OP common)
Platypelloid = Poor (3-5%, flat, deep arrest)
🎯 The 5 Critical Measurements:
- Diagonal Conjugate: ≥12.5cm (clinical measurement)
- Obstetric Conjugate: ≥10cm (calculated from DC)
- Interspinous: ≥10cm (midplane, smallest!)
- Intertuberous: ≥11cm (outlet)
- External Conjugate: ≥20cm (predictive)
🎯 Clinical Assessment Rules:
- Measure DC in early pregnancy (before engagement)
- Never do internal pelvimetry if placenta previa suspected
- Android features = Refer for hospital delivery
- Contracted midplane = Anticipate instrumental delivery/CS
- Document all findings in ANC card
⚠️ FINAL EXAM TIP: Android pelvis is MOST COMMON cause of CPD in Uganda due to nutritional/genetic factors. Early identification = life-saving referral!
"The pelvis is the baby's first home. Know its shape, predict the journey, and guide the mother safely to delivery!"
"For You created my inmost being; You knit me together in my mother's womb." - Psalm 139:13