
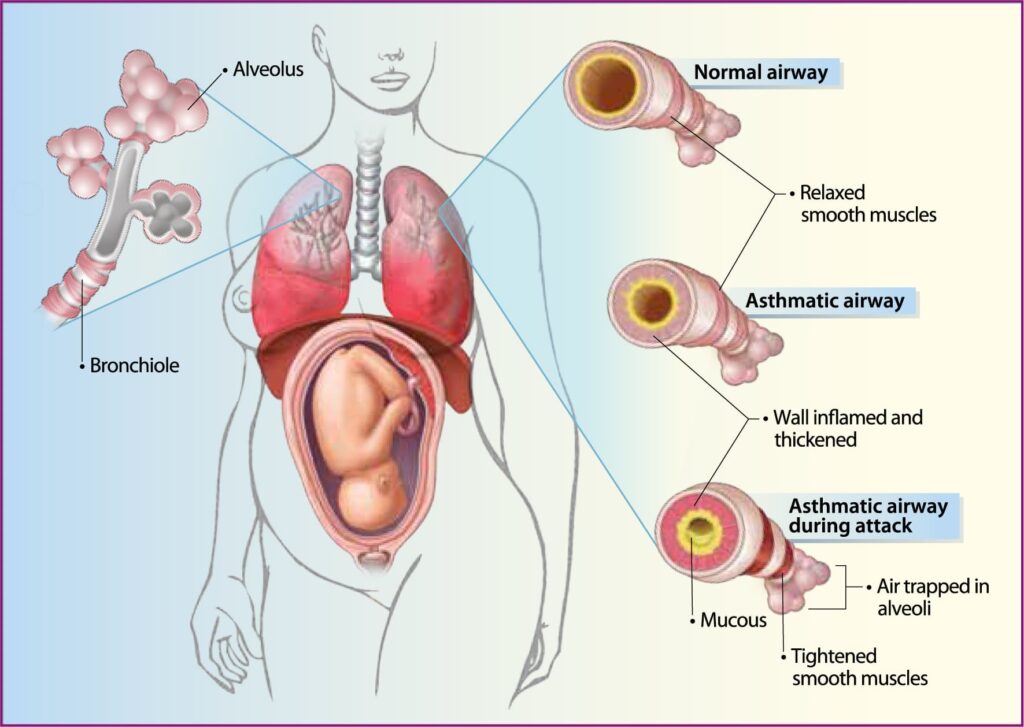
Management of Asthma in Pregnancy
Aims of Management
- Control symptoms, including nocturnal symptoms.
- Prevent acute exacerbations.
- Ensure no limitations on activities.
- Maintain (near) normal pulmonary function.
- Protect the mother and fetus from adverse effects.
Preventive Measures
When the patient is not experiencing an attack, prevention is very important. The following advice is given:
- Education: Inform the patient about asthma and identify potential triggers.
- Avoidance of Triggers: Avoid substances that trigger attacks (varies by individual).
- Warm Clothing: Use warm clothes, such as scarves, in cold weather.
- Emotional Control: Learn to manage emotions to prevent attacks.
- Deep Breathing Exercises: Practice exercises to ensure full lung expansion.
- Medication: Always have a supply of prescribed drugs (e.g., inhalers) according to the prescriptions.
Emergency Management
If the patient is experiencing an attack, treat it as an emergency:
- Admission: Quickly admit the patient in an upright position and administer oxygen if available.
- Reassurance: Reassure the patient and relatives to reduce anxiety, which can exacerbate the condition.
- Ventilation: Ensure proper ventilation and inform the doctor.
- Medical Treatment:
- Bronchodilators: Administer intravenous Aminophylline (250-500mg every 8 hours, given slowly over 20 minutes). Nebulized salbutamol (4mg every 8 hours), which may later be replaced with ordinary inhalers.
- Corticosteroids: Hydrocortisone (100mg intravenously every 8 hours), later changed to oral prednisolone.
- Antihistamines: Piriton or Phenergan to reduce allergic reactions and congestion.
- Antibiotics: Crystalline penicillin (2ml every 6 hours) or Ampicillin (500mg every 6 hours) to prevent or treat respiratory infections.
- Intravenous Fluids: Administer dextrose 5% to prevent dehydration and provide energy.
Quick Relief for All Patients
- Short-acting bronchodilator: 2-4 puffs of short-acting inhaled beta-agonist(Such as Salbutamol) as needed for symptoms. Intensity of treatment depends on the severity of exacerbation; up to 3 times at 20-minute intervals or a single nebulizer treatment as needed. A course of systemic corticosteroids may be needed. Use of short-acting inhaled beta-agonist more than 2 times a week in intermittent asthma (daily, or increasing use in persistent asthma) may indicate the need to initiate or increase long-term control therapy.
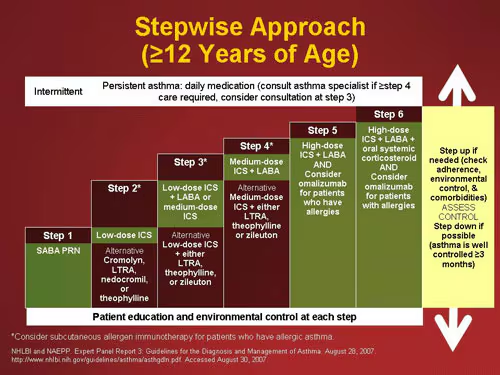
Step Ladder Management
- Step 1: Occasional use of inhaled short-acting beta2-adrenoceptor agonist bronchodilators.
- Step 2: Introduction of regular preventer therapy, preferably inhaled corticosteroids (ICS).
- Step 3: Add-on therapy with long-acting beta2-agonists (LABAs), such as salmeterol and formoterol.
- Step 4: Poor control with Step 3: Addition of a fourth drug, such as leukotriene receptor antagonists or theophyllines.
- Step 5: Continuous or frequent use of oral steroids.
Non-Pharmacological Management
Patient Education
- Explain that it is safer for pregnant women with asthma to take asthma medications than to have ongoing symptoms or exacerbations.
- Reassure that safe and adequate asthma treatment is possible during pregnancy and that good asthma control minimizes the risk of complications.
Smoking Cessation
- Smoking increases the risk of asthma exacerbations, bronchitis, or sinusitis, and necessitates an increased need for medication.
- Associated with adverse pregnancy outcomes, including spontaneous pregnancy loss, placental abruption, preterm premature rupture of membranes (PPROM), placenta previa, preterm labor and delivery, low birth weight, and ectopic pregnancy.
Control of Environmental Triggers
- Reduce the need for pharmacologic intervention by avoiding exposure to allergens and nonspecific airway irritants like tobacco smoke, dust, and environmental pollutants.
- Particular allergens of concern include dander from pets and antigens from household dust mites.
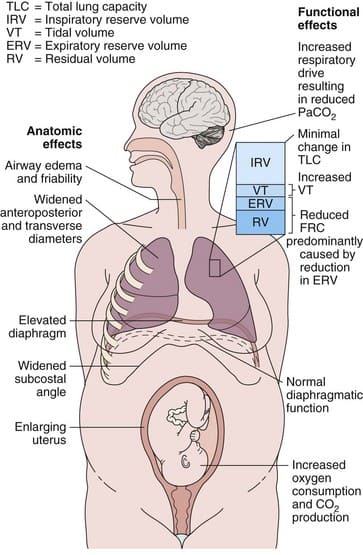
Nursing Care
Bed Rest: Complete bed rest is essential, with assistance provided for all activities due to dyspnea.
- Maternal Positioning: Pregnant patients with acute asthma should rest in a seated or lateral position to avoid aortocaval compression by the gravid uterus, particularly in the third trimester.
- Hydration: Intravenous fluids are not necessary unless the patient cannot maintain oral hydration.
- Supplemental Oxygen: Initially 3 to 4 L/min by nasal cannula, adjusting to maintain a PaO2 of at least 70 mmHg and/or oxygen saturation of 95% or greater.
Observation: Monitor fetal condition and mother’s response to treatment closely.
